Tzar Oluigbo (Lead writer)
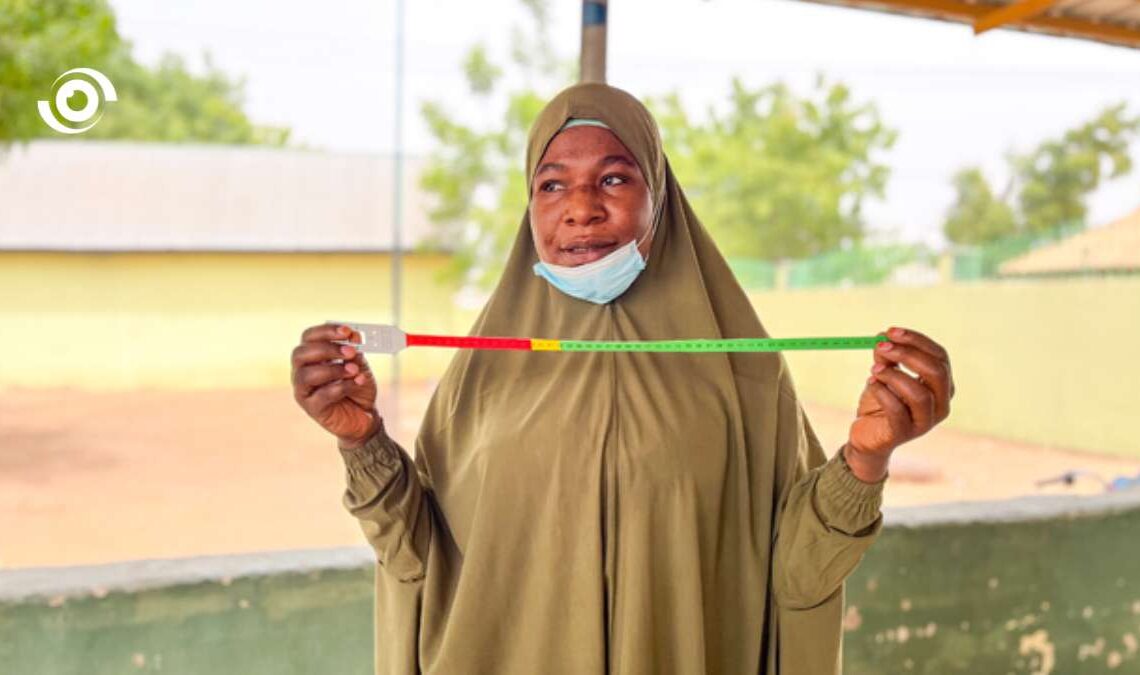
When 16-month-old Babangida was brought to the Taimaka outpatient clinic in Yamaltu-Deba Local Government Area of Gombe State, he was already severely malnourished. His mother, Asmau, was only 19. By the time they arrived at the health facility, the concern was visible in his tiny body, evident in the urgency of the assessment by the health workers, uncertain what would happen next.
He weighed 4.4 kg on arrival. Health workers measured his mid-upper arm circumference (MUAC) at 8.4 cm, a value indicating severe acute malnutrition (SAM). He was then started on treatment with Ready-to-Use Therapeutic Food (RUTF). “I was scared I would lose him, but I kept coming because I wanted him to live,” said Asmau, adding that “as a mother, I couldn’t give up on him. No matter how hard it was, I kept coming.”By the end of his 12-week treatment, his weight had increased to 7 kg and his MUAC to 12.5 cm.
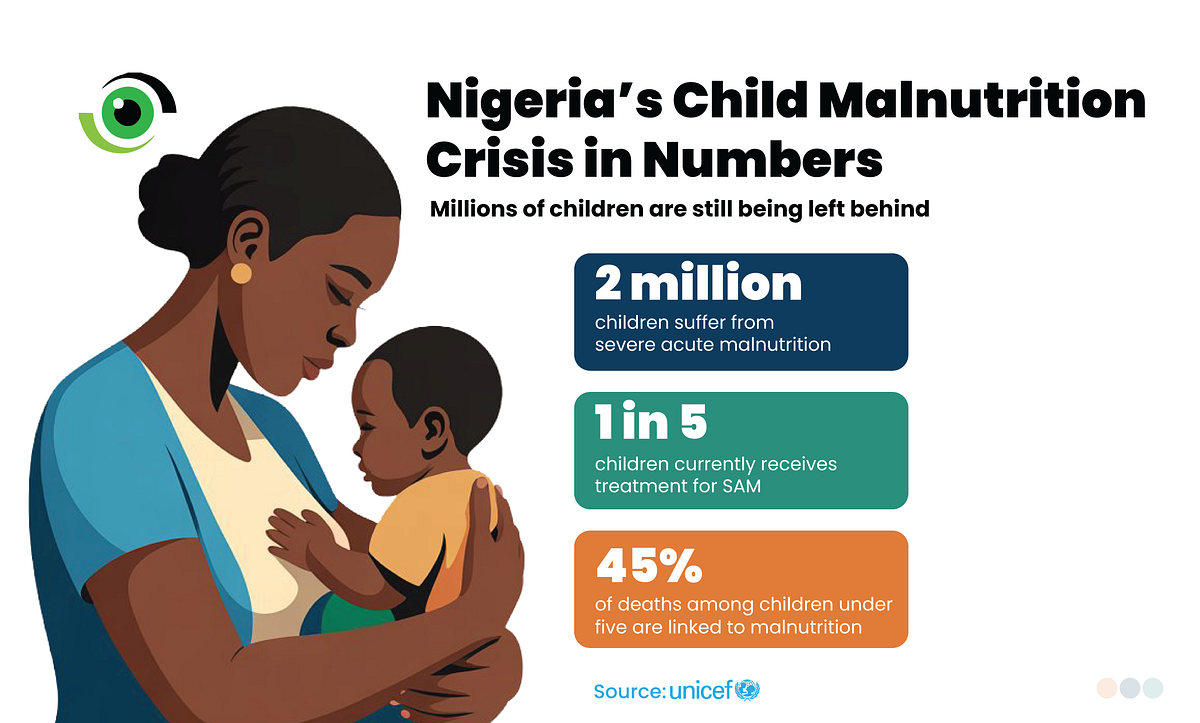
The latest joint estimates from the World Health Organization (WHO), UNICEF, and the World Bank show that 42.8 million children under five were affected by wasting globally in 2024, including 12.2 million with severe wasting. In Nigeria, about 2 million children suffer from severe acute malnutrition, but only around two in ten currently receive treatment. Malnutrition also remains a direct or underlying cause of 45 per cent of under-five deaths.
That is the gap Taimaka aims to bridge. Founded in 2019, the organisation later shifted to malnutrition treatment and now operates through government-linked facilities in Gombe State. Taimaka states it has treated over 12,000 children and developed a model that depends on digitally supported community health workers and more affordable delivery methods. “At the end of the day, what we care about is how many children are alive because of what we have done,” Dr Justin Graham, co-founder of Taimaka, said. “What we do is not just nutrition, it is paediatric healthcare.”
Currently, Taimaka operates primarily in two LGAs in Gombe State; Yamaltu-Deba and Funakaye (with ongoing expansion to Dukku), with 14 outpatient clinics and 2 in-patient facilities at the General Hospitals of both LGAs, providing over 200 beds and caring for more than ten thousand children each year, many of whom would otherwise not survive.
Bringing treatment closer to families
The essence of Taimaka’s model involves a fundamental shift. Care is brought closer to the communities where children live, rather than relying only on distant hospital-based treatment. Children are screened using MUAC and assessed for clinical stability. Those who are alert, able to feed, and free of serious medical complications can usually be managed as outpatients. Those with poor appetite, severe oedema, danger signs, or additional complications require inpatient care.

The model also recognises that malnutrition rarely occurs in isolation. Infections and undernutrition reinforce one another, and illnesses such as diarrhoea can worsen nutritional decline. According to Dr Abubakar Umar, the co-founder of the organisation, “we leverage existing structures and use technology to guide care. With the app, a trained health worker can assess a child and get a clear management plan without needing a physician at every point.” That matters in settings where specialist staff are limited, and delays can be deadly.
For uncomplicated severe acute malnutrition, the standard therapeutic product remains ready-to-use therapeutic food (RUTF). UNICEF guidance describes RUTF as a ready-to-eat, high-energy fortified food used for children aged 6 to 59 months with severe wasting, no medical complications, and appetite. Taimaka has also explored simplified treatment ideas linked to the Optimizing the Management of Acute Malnutrition (OptiMA) approach, which uses MUAC and oedema for admission and progressively reduces RUTF dosage as a child improves. “Using less to reach more is one of the ways we maximise impact,” Dr Graham explained.

Image credit: Nigeria Health Watch
Taimaka has also tested Tom Brown, a locally produced mix of grains and legumes, in work related to moderate acute malnutrition. That distinction is significant. Locally produced supplementary foods may assist in moderate cases of malnutrition or for relapse prevention, but they should not be mistaken for RUTF’s standard role in treating severe acute malnutrition.
From outpatient care to critical care
At the frontline are the outpatient therapeutic programmes (OTPs), embedded within primary health care (PHC) centres. This is where most children with severe acute malnutrition are first identified and treated. “As soon as a child is brought in, they are assessed at the outpatient clinic and started on RUTFs,” explained Dr Timothy Benjamin Meller, the inpatient therapeutic programme manager. “But if the child cannot tolerate it, or presents with complications like diarrhoea, vomiting, convulsions, or oedema, they are immediately referred to the inpatient therapeutic programme.”
The inpatient therapeutic programme (ITP) functions as a specialised paediatric hospital for the most critical cases. Children admitted here have SAM and medical complications requiring additional care. “The ITP is essentially a hospital setting where we manage critical cases,” Dr Meller said. “We have an emergency ward, an acute ward, and a transition ward. Children are triaged according to the severity of their condition. Some require oxygen, while others may need a blood transfusion. The aim is to stabilise them as quickly as possible.”
Treatment in ITP follows a carefully staged process. Children are initially stabilised with therapeutic milk (F-75), designed for those in fragile condition. As they improve, they are moved to F-100, a higher-calorie formulation that supports recovery and weight gain. Once stabilised, they are transitioned back to outpatient care. After discharge, children return to the OTPs where they continue treatment with RUTF over a standard 12-week period, ensuring continuity of care and close monitoring.
“For us, it is a continuous system,” Dr Meller added. “For those in the inpatient unit, if they fail to stabilise or their condition remains critical despite treatment, we escalate care by referring them to teaching hospitals for more advanced medical intervention.”

Challenges, community realities, and the road ahead
Even the best-designed treatment model faces limitations when children arrive too late. “Many children present very late,” Dr Umar noted. “By the time they arrive, the condition is already severe.” That is not only a clinical issue, Delays in seeking care can be influenced by costs, distance, household pressures, and beliefs about illness and treatment. Research from Nigeria has demonstrated that caregivers’ health beliefs can affect whether and when they access facility-based care for sick children.
That is why the lesson from this model extends beyond a single clinic or organisation. Treatment must be integrated within a broader system that includes community screening, caregiver counselling, trust-building, referral pathways, and preventive nutrition support. Recent reports from Gombe show that the state is also attempting to enhance prevention by training health workers and better supporting mothers before children fall into severe illness.
The question beyond impact: can it last?
The most important test now is not whether the model can save children one by one, but whether it can be sustained, funded, and integrated into more established routine care. “We’re all philanthropically funded, which is always a difficulty,” said Dr Graham. “Our goal is to ensure we never grow at a rate that is unsustainable; we want to at least maintain the size of the programme year on year.”
Looking ahead, Taimaka’s goal is to treat at least 100,000 SAM cases each year over the next five years, with plans to expand into other Nigerian states. Meanwhile, Dr Graham emphasised that the organisation’s focus is on outcomes and not just activity levels. “The core metric that we track is the number of lives that we save,” he said. “At the end of the day, what matters is how many children are alive because of what we have done.”