


Ibukun Oguntola and Chinwendu Iroegbu (Lead writers)
In this latest edition of Nigeria Health Watch’s Curated Conversations, the Country Representative of the World Health Organization (WHO) Nigeria, Dr Pavel Ursu, discusses what it takes to transform Nigeria’s primary health care (PHC) system from vision into reality. His conversation with Nigeria Health Watch comes at a time when there is a clearer effort to align and coordinate health reforms across the sector, even as the depth of the challenges facing the health system remains evident and significant work is required to address them.
During the discussion, Dr Ursu emphasised that Nigeria will not achieve universal health coverage (UHC) through policy alone. It will happen only if primary health care becomes functional, trusted, and sustainable enough for people to actually seek care. He noted, “Without Nigeria accelerating, we cannot reach those targets which everybody agreed we have to reach within the UHC and health security agenda in the world.”


WHO officially announced Dr Ursu as its Representative to Nigeria in October 2025, highlighting Nigeria as home to its largest country office in Africa, and reflecting Nigeria’s strategic role in regional and global health progress. WHO has consistently described PHC as the backbone of a resilient health system, reinforcing why it remains the most appropriate starting point for reform.
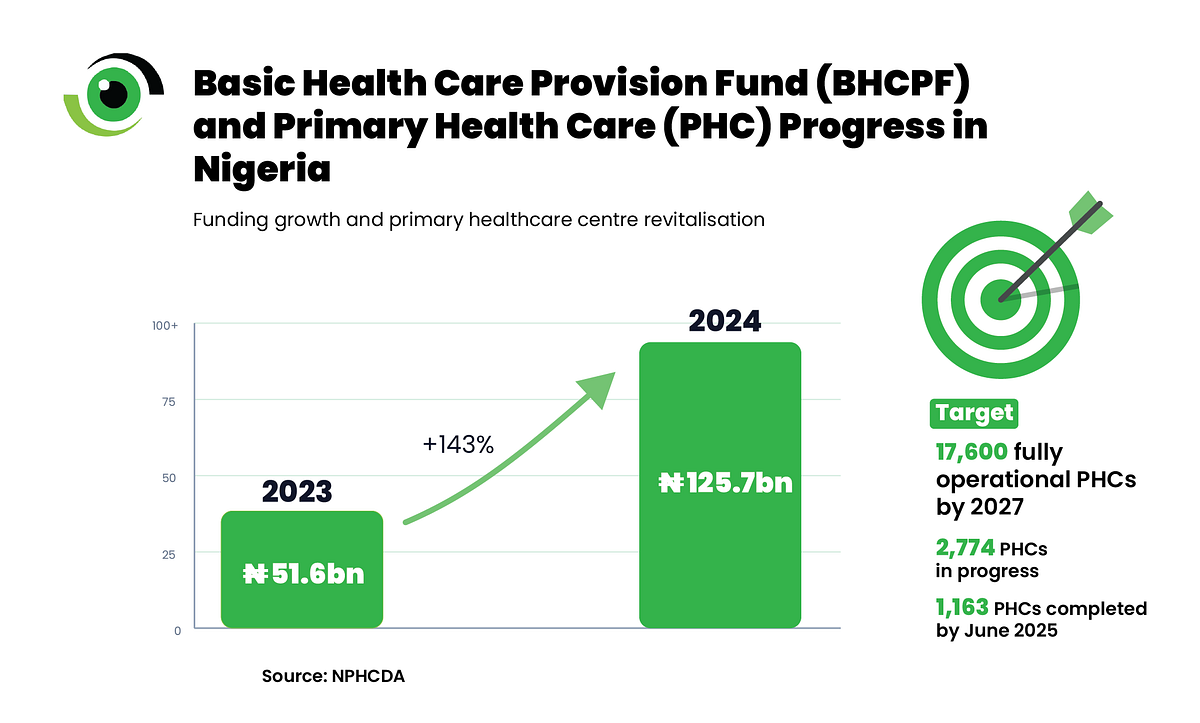
The National Primary Health Care Development Agency (NPHCDA) reports that PHC revitalisation is ongoing, with 1,163 facilities completed by June 2025, 2,774 more in progress, and a target of 17,600 fully operational PHCs by 2027. The issue is not the absence of policy, but the challenge of translating intent into sustained system performance, as the sector works to move beyond long-standing underperformance towards a more structured recovery.
Dr Ursu does not describe Nigeria’s challenge as a lack of vision but as an issue of alignment. “There is no lack of vision, planning, wisdom, or capacity, even in terms of the knowledge around primary health care,” he noted. Nigeria has no shortage of policies, strategies, technical working groups, or reforms. What it has struggled with over time is fragmentation, with funding flowing through multiple channels that do not always reinforce one another.
The fragmentation shows up in different ways. Infrastructure may improve without the same attention to staffing and supplies, while data systems are often stronger at collecting information than at informing decision-making. The current reform framework is at least beginning to address these gaps. Under the Nigerian Health Sector Renewal Investment Initiative launched in December 2023, the federal government has introduced a Sector-Wide Approach centred on “one plan, one budget, one conversation.”
That effort becomes even more important as the external funding environment continues to tighten. While donor support represents a relatively small share of overall health funding, it still funds many interventions that governments have historically underfunded. The challenge, therefore, is not that donor funding is declining, but that its reduction exposes the risks of sustaining essential health functions through fragmented, semi-parallel systems. Dr Ursu emphasised the need for a more deliberate approach, noting that “it is not for us to do more with less, but to really engage strategically and always incorporate system thinking and sustainability into our interventions.”

This is where the Basic Health Care Provision Fund (BHCPF) becomes more than just a budget line. Funding increased from ₦51.6 billion in 2023 to₦125.7 billion in 2024, reinforcing its role as one of Nigeria’s most important domestic PHC financing platforms. More than 8,300 validated PHCs are now receiving quarterly direct facility funding. The real question, however, is whether BHCPF functions as intended with funds released on time, facilities using them effectively, communities able to track performance, and systems in place to ensure transparency and reward results.
Nigeria continues to face high out-of-pocket expenses, with World Bank data indicating that household payments account for 71.9% of current health expenditure. This is why PHC reform cannot be assessed solely by the number of renovated buildings or retrained staff. A health system can expand services on paper and still fall short if care remains financially out of reach at the point of use. A PHC-led UHC strategy that does not lessen that burden will remain incomplete.

Dr Ursu also emphasised trust as a central element of reform, framing it as something built through participation rather than instruction. “It is not top-down solution creation, it is co-creation of the solution with the community. And this is how trust is then established between the community and the providers.” Nigeria already has community-facing structures that can help translate trust into a practical tool, such as Ward Development Committees, the Community Health Influencers Promoters and Services (CHIPS) programme, and the involvement of traditional and religious leaders in reform efforts.
The federal government has described these leaders as trusted allies who can help reach communities that formal systems often struggle to access. Trust is not built through policy statements alone. It is earned when local facilities are open, respectful, well-stocked, accountable, and visibly connected to the communities they serve. Dr Ursu also highlights an important gap in how health systems are often analysed, “We are used to looking at the gaps, what is not available, and less observant of the strengths in the community.” In Nigeria, those community strengths matter.
One of the clearest messages from the conversation with Dr Ursu is not that Nigeria needs more ideas, but that it needs to focus on delivering on what already exists. The country’s reform agenda now includes several important frameworks, including the Sector-Wide Approach (SWAp) and BHCPF, as well as PHC revitalization, community platforms, workforce reforms, and health-security planning. Dr Ursu described SWAp as “a genuine structural shift” and “a pathway to achieve sustainability and domestic funding through this transition.”

That assessment matters because the SWAp is designed to reduce fragmentation, align partners around a shared direction, and strengthen accountability across different levels of the system. If implemented with intent, this kind of reform architecture can help shift the country away from a collection of disconnected interventions towards a more coordinated and functional public health system.
The more important question is whether federal, state, and local actors can coordinate these tools long enough for Nigerians to experience a tangible difference. That is when primary health care moves beyond a slogan and becomes the true frontline of care. It is when UHC shifts from a target to a public commitment that people can recognise and trust.
That is why Dr Ursu’s closing point resonates. “There is no other solution, no one is there to solve the problems in a sustainable manner except people who show leadership, who know that their family and their community are there.” That is the moment Nigeria faces now, both a challenge and a clear opportunity.