


Solomon Yemi Oladimeji (Lead writer)
In Nigeria’s federal health system, the question of who pays for healthcare is just as important as who delivers it. While national policies often dominate discussions on health sector reform, many of the decisions that ultimately shape access to healthcare are made in state budgets.
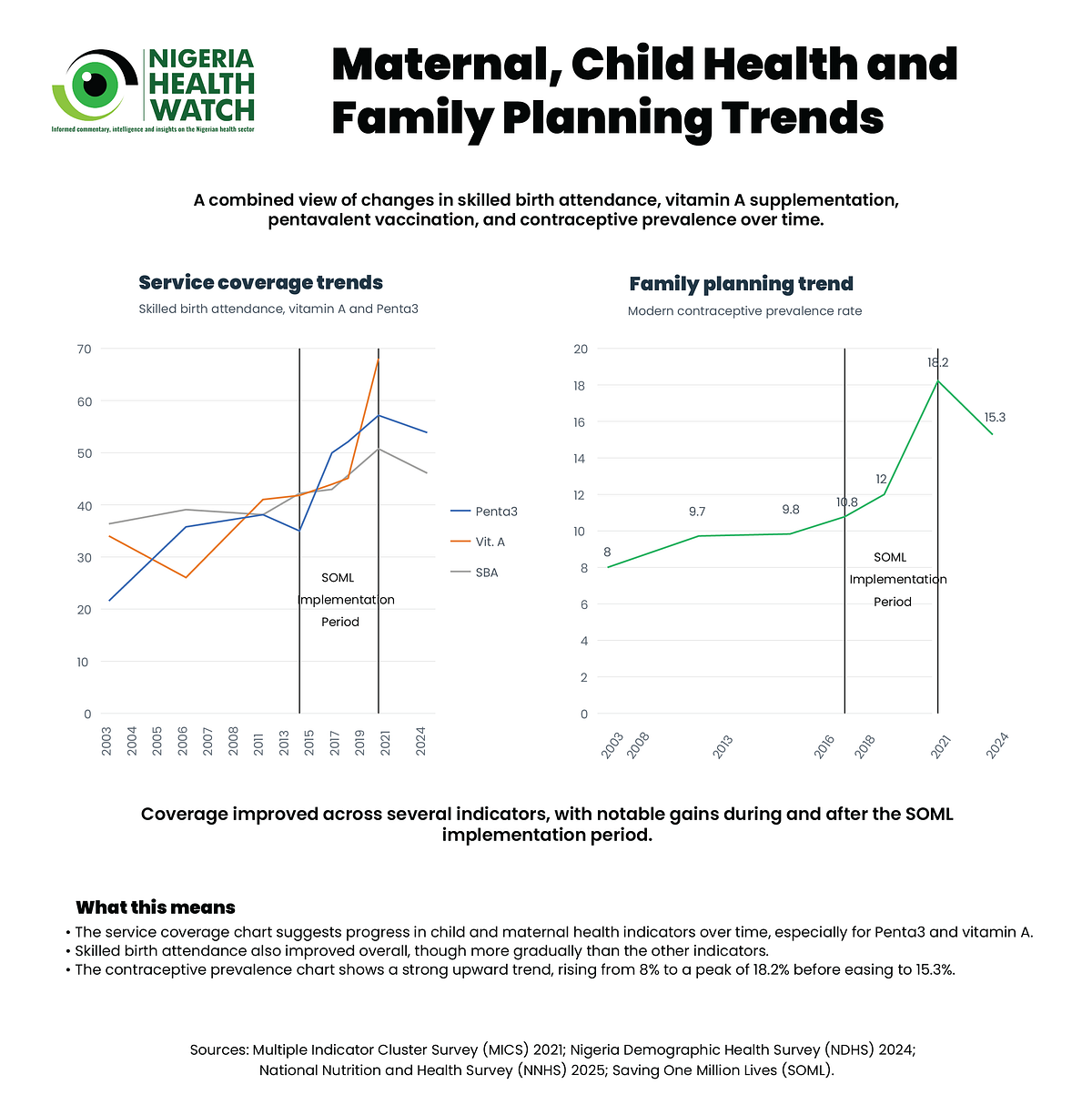
Between 2016 and 2021, Nigeria implemented one of the most ambitious results-based financing experiments in its health sector, the Saving One Million Lives Programme for Results (SOML-PforR). Supported by the World Bank’s Program-for-Results financial instrument, the programme linked federal disbursements to states with independently verified improvements in key maternal and child health indicators. States received financial rewards for measurable progress across priority areas, including immunisation coverage, maternal care utilisation, nutrition interventions, and improvements in health system performance.
Evidence from the SOML-PforR evaluation suggests that these incentives contributed to meaningful improvements in service delivery across several of these indicators. National coverage of the third dose of the pentavalent vaccine increased by more than 20% points during the programme period; Vitamin A supplementation expanded across multiple states; and facility readiness indicators improved.
Importantly, the programme also helped narrow performance gaps across states, with poorer-performing states registering some of the largest improvements. This equity effect was particularly notable. States that started with lower baseline coverage often experienced faster improvements, suggesting that performance-linked financing can help accelerate progress where health systems are weakest. While SOML-PforR did not solve Nigeria’s health system challenges, it demonstrated an important principle: financial incentives can influence state-level policy choices in a federal health system.

States now finance a growing share of Nigeria’s health system
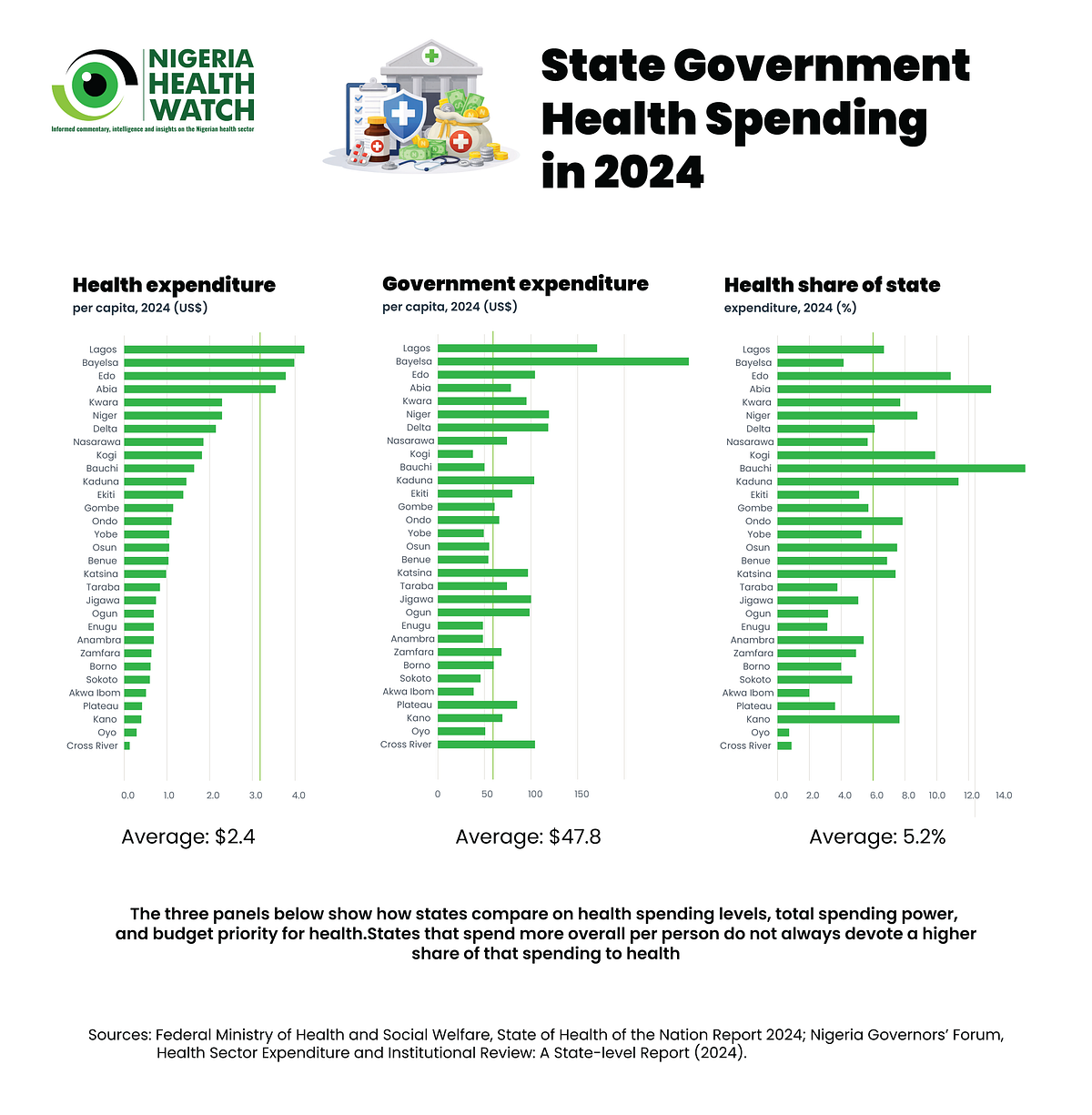
Recent analysis by the Nigeria Health Commissioners Forum and TEKANO Group shows that states accounted for approximately 39.3% of government health spending in 2024, spending an average of about US$2.4 per capita on health, a level that reflects the persistent underfunding of health systems.
The government spend on health represents a substantial increase from previous years, when state spending accounted for roughly 30% of total government health spending in 2022 and 24.9% in 2023. These figures reflect an important structural reality in Nigeria’s federal system: states are now the primary financiers of primary and secondary healthcare services, which are the main entry points for most Nigerians seeking care.
At the same time, the federal government’s role in health spending remains heavily concentrated in tertiary care and administrative functions. In 2024, more than 80% of federal government health expenditure was directed toward administration and tertiary healthcare institutions, leaving states responsible for much of the financing needed to sustain frontline service delivery.
By international comparison, however, Nigeria’s public spending on health remains extremely low. According to the World Health Organization (WHO) Global Health Expenditure Database, government health expenditure stood at roughly US$12 per capita in 2023, far below the average of approximately US$55 among countries with similar income levels in sub-Saharan Africa, and significantly lower than the estimated US$90 per capita associated with progress toward health-related Sustainable Development Goals. This overall financing gap means that decisions taken within state budgets carry even greater weight in determining whether frontline health services are adequately funded.


Large and persistent spending disparities across states
Despite the growing role of states in financing health services, the distribution of spending across states remains highly uneven. Across Nigeria, state government health expenditure per capita ranges from approximately US$0.4 to US$5.9, representing a more than ten-fold difference between the lowest- and highest-spending states. These disparities are not driven solely by differences in fiscal capacity. Two factors largely explain the variation in health spending across states:
- Differences in the overall size of state government spending
2. Differences in how much priority states assign to health within their budgets
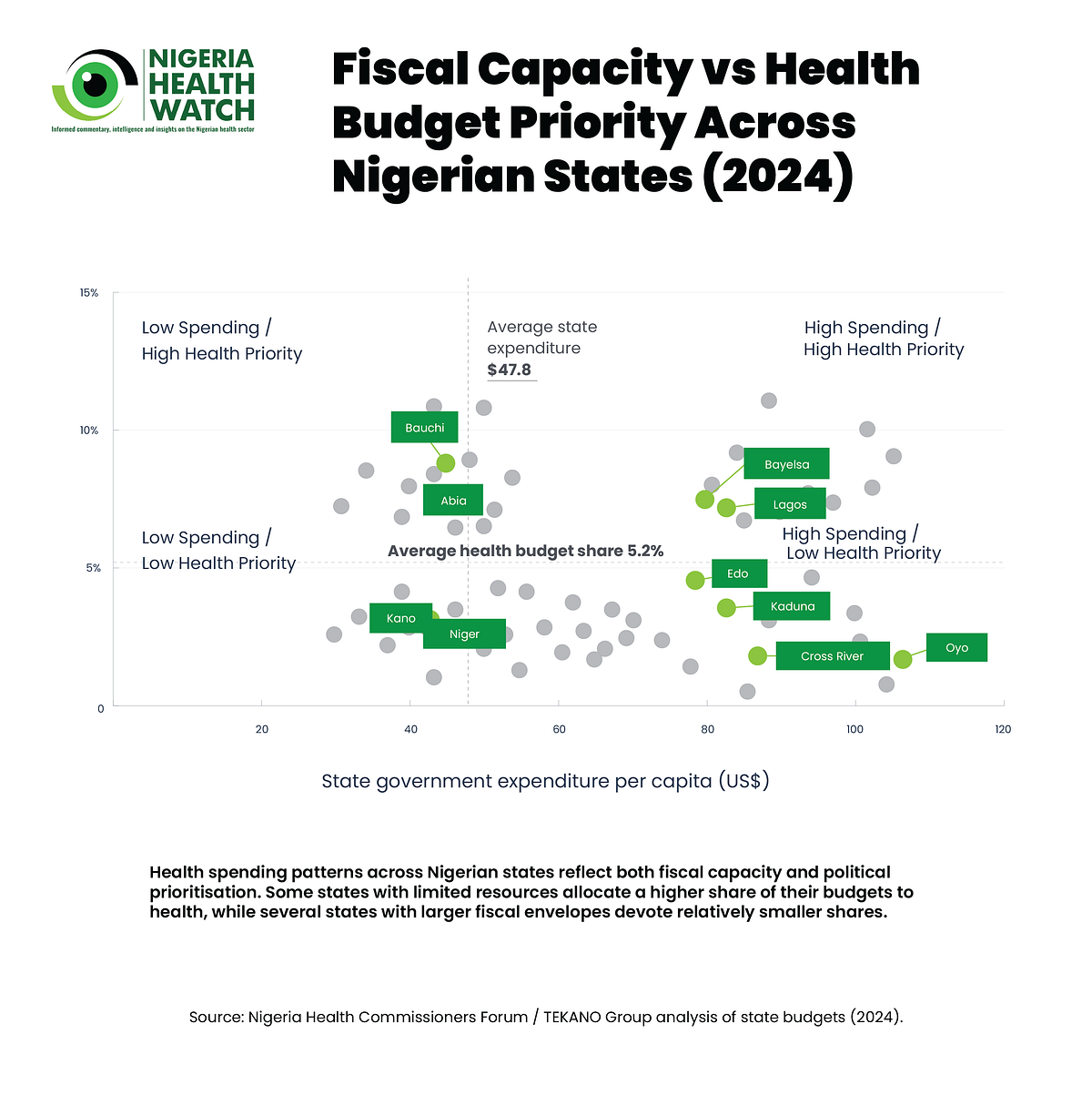
Between 2022 and 2024, state fiscal envelopes expanded significantly. Average state government expenditure per capita increased from US$26.6 in 2022 to US$31.6 in 2023 and then rose sharply to US$47.9 in 2024. However, this expansion in overall spending has not translated into increased prioritisation of the health sector. Over the same period, the average share of state government expenditure allocated to health declined from 7.3% in 2022 to 6.0% in 2023 and further to 5.2% in 2024.
The variation in health prioritisation across states is particularly striking. In some states, health accounts for less than 1% of total government expenditure, while in others it exceeds 13%. This more than twenty-fold variation suggests that health spending patterns are shaped not only by fiscal capacity but also by political and policy choices made within state governments.
These choices ultimately determine whether resources reach primary healthcare facilities, whether vaccines are available in communities, and whether frontline health workers receive adequate support.
These disparities have significant implications for equity. In practice, access to essential health services, including whether a pregnant woman can obtain antenatal care, whether vaccines are consistently available in primary health care (PHC) facilities, and whether community health workers are adequately supported, increasingly depends on where Nigerians live rather than on a consistent national standard of care.
The missing link between financing and health results
As states assume an increasingly central role in financing healthcare, the question of how to ensure accountability for results becomes more important.
During the SOML-PforR implementation period, performance-based grants provided a mechanism to align financing with measurable health outcomes.
States that improved coverage or strengthened service delivery were rewarded with additional funding, creating an incentive structure that encouraged policy attention to maternal and child health indicators. Today, however, Nigeria’s health financing architecture relies more heavily on traditional budgetary allocations and conditional grants, including the Basic Health Care Provision Fund (BHCPF). While these mechanisms play an important role in financing primary healthcare, they do not always embed strong performance incentives linked directly to measurable outcomes.
At the same time, new reforms under the Health Sector Renewal Investment Initiative (NHSRII) and the government’s 4-Point Agenda seek to strengthen governance, expand equitable access to quality healthcare, unlock the health value chain, and enhance health security. These reforms provide an important opportunity to rethink how financing flows can reinforce accountability for measurable results within Nigeria’s federal health system.
Why state budget choices will determine reform success
Ultimately, the success of Nigeria’s current reform agenda will depend not only on national policy frameworks but also on decisions taken within state budgets. If states are now responsible for nearly 40% of government health spending, then their budget priorities will play a decisive role in determining whether Nigeria achieves sustained improvements in maternal and child health outcomes. States with larger fiscal envelopes but low health budget shares may struggle to expand service coverage, while those that prioritise health spending are more likely to strengthen primary healthcare systems and improve access to essential services.
This reality underscores the need to restore results-based discipline within Nigeria’s evolving health financing architecture. Rather than replicating SOML-PforR exactly as it existed before, Nigeria’s reform agenda could incorporate elements of performance-linked financing into newer funding mechanisms. Conditional grants, federal transfers, and other financing instruments could be structured to reward measurable progress in service coverage, equity, and health system performance. Such an approach would reinforce the principle that greater state responsibility must be matched with stronger accountability for results.
Ekiti State offers a practical example of how this can work. The Ministry of Health and Human Services established a clear accountability framework linking inputs, outputs, and outcomes across the sector. Working with agencies including the drug supply management agency, hospital management board, and the state health insurance scheme, the Ministry aligned efforts around a shared UHC strategy.
Weekly review meetings chaired by the Commissioner tracked progress and addressed operational challenges, while engagement with legislators helped sustain support during budget negotiations. This approach strengthened confidence in the sector’s performance and contributed to allocations for agencies delivering essential services rising from 13 percent of the health budget in 2019 to 41 percent in 2025.
A Federal Health System Where Both States and Results Matter
Nigeria’s health system operates within a complex federal structure in which authority, financing, and service-delivery responsibilities are distributed across multiple levels of government. As states assume a growing role in financing healthcare services, ensuring that resources translate into measurable health outcomes becomes even more critical.
The experience of SOML-PforR demonstrated that performance-based incentives can help drive improvements in coverage, equity, and service delivery. The priority now is not to replicate the programme in its previous form, but to ensure that the discipline of results-based accountability remains embedded in Nigeria’s health financing system.
As Nigeria advances the Nigeria Health Sector Renewal Investment Initiative (NHSRII) and its 4-Point Agenda, the real test of reform will not lie solely in national strategies or policy commitments, but in the budgetary decisions taken across Nigeria’s 36 states. Whether states increase the share of their spending devoted to health, strengthen primary healthcare systems, and align financing with measurable outcomes will ultimately determine whether the country translates reform ambition into tangible health gains. In a federal health system where states matter more than ever, ensuring that results matter just as much may prove to be the most important reform of all.