


Hadiza Mohammed and Onyedikachi Ewe (Lead writers)
Success, 13, did not panic when she got her first period. ‘I was educated early,’ she recalled, ‘I simply used a sanitary pad and carried on with my day.’ In many Nigerian communities, that kind of confidence is still not common for girls entering puberty. Success is a student at a school in the Jiwa community, a peri-urban area in Nigeria’s Federal Capital Territory (FCT), where more girls are beginning to speak openly about their experiences as they start puberty.
Despite growing public attention to sexual and reproductive health, many adolescents still lack accurate information about puberty, consent, bodily autonomy, and where to seek help if they experience sexual abuse. To help close this gap, the Centre for Family Health Initiative (CFHI), a community-based organisation working in the FCT, runs a year-long programme for girls aged 9 to 17.
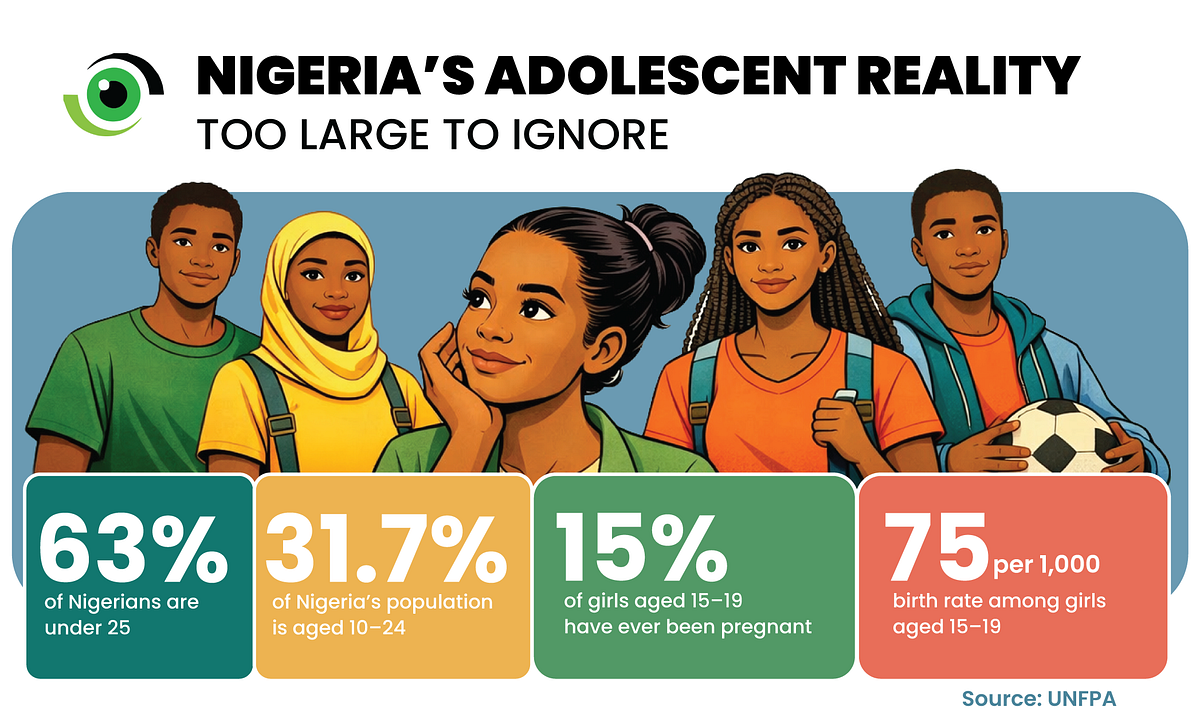
Nigeria’s young population makes adolescent health an urgent policy priority. According to the United Nations Population Fund (UNFPA), young people aged 10 to 24 make up 31.7 per cent of the population, while 63 per cent of Nigerians are under 25. The need is urgent. About 15 per cent of girls aged 15 to 19 have ever been pregnant, with a birth rate of 75 per 1,000 among girls in that age group.
In the FCT, these risks are complicated by weak school-to-health facility linkages, stigma, and limited access to accurate information. Nationally, 46 per cent of girls and young women aged 15 to 24 are sexually active, while 8 per cent report having had sex before the age of 15.

Built on community trust
Instead of approaching schools directly to introduce sexual and reproductive health interventions, CFHI begins by engaging traditional rulers in each community. Princess. E. Okhaifoh, Programme Officer at CFHI, explains that this step is essential. ‘We cannot enter a community and start talking about sexuality with young girls without first earning the trust of the gatekeepers,’ she said, explaining that ‘once the traditional ruler understands our purpose, it helps reduce suspicion and resistance.’
According to Tanko Nuhu, Madaki of Jiwa community and the PTA chairman of Junior Secondary School Jiwa, ‘when CFHI came to our community, they first sought the Emir’s permission, clearly explaining their goals around sexual and reproductive health education. We welcomed their initiative and shared the information with the schools they planned to visit.’
Once approval is granted, CFHI partners with selected secondary schools and caregivers to run structured weekly sessions with first-year students through the Dreams Girls programme. The focus on first-year students is deliberate. ‘We want to reach them early, before misinformation spreads, before peer pressure intensifies, and before certain risks escalate,’ explained Okhaifoh.
In addition to the Dreams Girls programme, which focuses on adolescent girls in schools, CFHI also runs Adolescent Clubs in communities that include both boys and girls. Through these initiatives, thousands of young people across communities in the FCT, such as Jiwa, Kuchingoro, Sabon Lugbe, Kabusa, and Karimo, have been reached and supported.
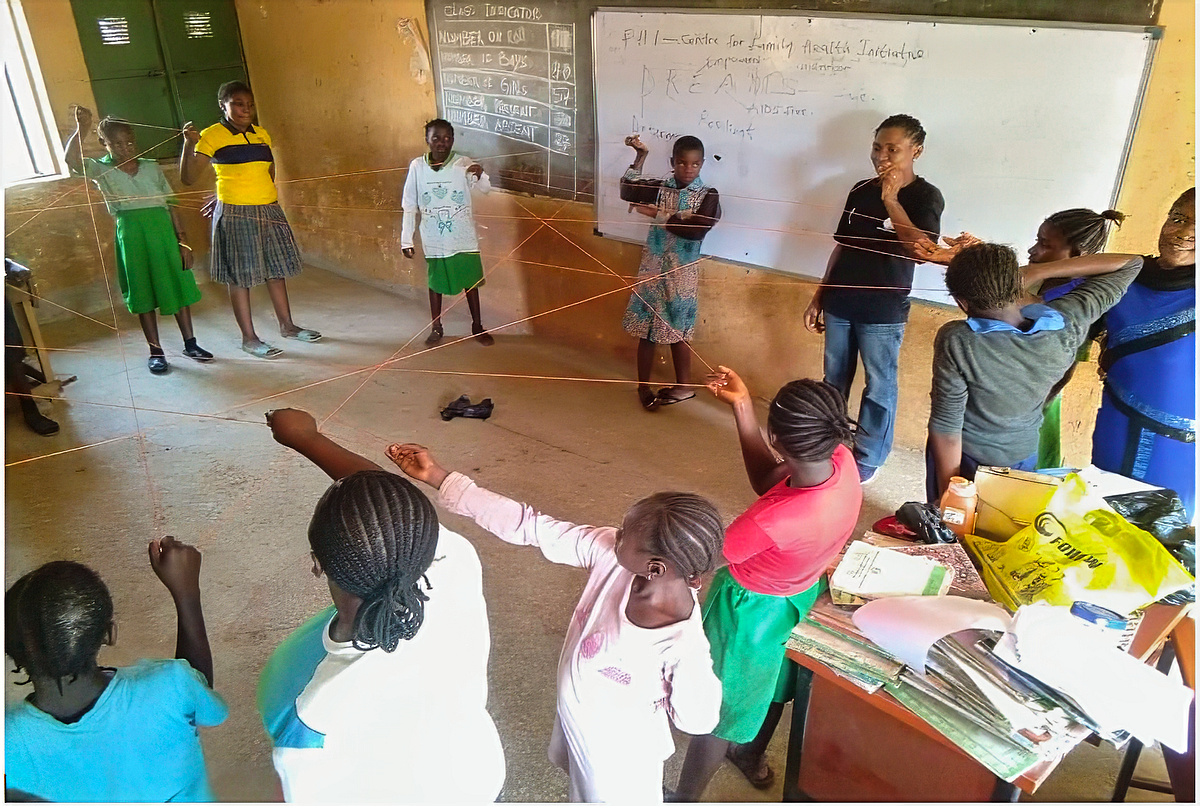
Over the course of one academic year, the girls learn about puberty, menstrual health management, consent, prevention of sexual abuse, HIV and other sexually transmitted infections (STIs), and where to seek help. The sessions are interactive, often using storytelling and role-play to make complex topics easier to understand and relate to.
Beyond classroom learning, CFHI has also supported improvements in school infrastructure. ‘Beyond teaching, they also made lasting improvements by building functional toilets, providing teachers’ tables, and supplying benches for the students. Their work has truly left a positive mark on girls and our schools,’ Nuhu noted.
CFHI also works closely with primary health care (PHC) in each community to link adolescent girls to counselling and health care services. Girls identified as particularly vulnerable, including survivors of abuse, people living with HIV, or those facing other reproductive health challenges, are referred confidentially to these centres to receive further support and care.
While the programme is still expanding, CFHI reports that from 2019 to date, it has reached 22 secondary schools across selected FCT communities, training hundreds of girls. Mrs Hauwa Usman, a teacher at Jiwa Secondary School, noted that more girls are now willing to report cases of harassment, ‘before, they would keep quiet. Now, some of them come forward.’
Caregivers are also noticing changes at home. One mother shared that her daughter now takes the lead in teaching her younger siblings and even her friends about sexual and reproductive health. “She talks to them about menstrual hygiene and personal safety,” the mother said with a smile. “It has strengthened communication in our home and given her so much confidence.”
For Success, the impact goes beyond her own experience. She now teaches more than twelve of her friends and siblings through peer-to-peer learning sessions on sexual and reproductive health. “Sometimes they ask me where I learned all this because the things I share help them understand their bodies better and know how to make safer decisions,” she noted.


For many of those around her, the information is not only new but practical, helping them navigate questions about puberty, hygiene, consent, and where to seek help when needed.
Why the model stands out
Adolescent sexual and reproductive health interventions are not new in Nigeria. What makes CFHI’s model notable is not that it is the only adolescent health intervention in Nigeria, but that it combines community gatekeeper engagement, sustained school-based sessions over an academic year, and clear links to nearby primary health care centres, three elements that are often separated.
First, the programme invests in community gatekeepers. By engaging traditional rulers before implementation, CFHI builds trust, reduces resistance, and creates a sense of local ownership. In settings where cultural and religious sensitivities shape how sexuality is discussed, this engagement helps make the programme more acceptable.
Second, the intervention runs across the entire academic year. This gives facilitators time to build trust with participants, revisit complex topics, and identify vulnerable cases over time. The integration with PHCs also strengthens the local health system by creating referral pathways that did not previously exist.
The programme also demonstrates the importance of linking the education and health sectors at the community level. Rather than operating in silos, schools and PHCs collaborate to address the multifaceted needs of adolescent girls.
CFHI has built strong partnerships with PHC facilities in Bwari and Abuja Municipal Area Council (AMAC), including Jiwa PHC and Gwagwa PHC, to ensure adolescents in schools can access sexual and reproductive health services. These partnerships combine formal agreements with advocacy visits, helping to build trust and keep collaboration running smoothly.

What stands in the way?
Despite promising progress, the programme faces several challenges. Schools often require formal letters from the Universal Basic Education Board (UBEB) before allowing student engagement, and in some cases, requests for bribes have been reported. Ensuring community ownership has also been difficult, as many schools do not continue the programme beyond the first year.
Additionally, funding constraints limit the number of schools CFHI can reach annually, and not all communities are immediately receptive. In some areas, discussions around consent and sexual violence remain sensitive, requiring careful facilitation.
Scaling the programme presents further hurdles. Expanding the model across the FCT or to other states would demand sustained funding, more trained facilitators, and stronger institutional partnerships with education authorities. Without these resources, broadening the reach while maintaining the quality of engagement and impact remains a significant challenge.
CFHI acknowledges these constraints. “We are seeing change at the community level,” Okhaifoh explained, “but to scale, we need more support and stronger systems.” For now, the impact is mostly visible in classrooms like Success’s, where silence is gradually giving way to conversation. “I used to be shy to talk about these things; now, I know it is about my health,” Success noted.
The lesson from Jiwa is not that one programme has solved adolescent sexual and reproductive health in the FCT. It is that when communities are brought in early, schools become more credible entry points, PHCs can be part of the response, and silence is more likely to give way to care.