

Women’s access to contraception has had a significant impact on societies, enabling them to have greater autonomy over their bodies, and the power to decide when and how many children they have. According to the 2018 Nigeria Demographic and Health Survey, the current met need for family planning is 19.9 percent for women in urban centres, and 9.6 percent for women in rural areas. 10.5 percent of women use a modern contraceptive method, with 40.8 percent of users sourcing them from private sector providers.

Task-Shifting Task-Sharing Policy in Nigeria
The task-shifting task-sharing policy for essential health care services in Nigeria was first approved in 2014 and updated in 2018. It presented an opportunity to increase access to family planning commodities and services through the lower cadre of health care workers such as community health extension workers. Despite the importance of private sector providers especially Community Pharmacists (CPs) and Patent and Proprietary Medicine Vendors (PPMVs) in healthcare provision at the community level, the policy failed to articulate a well-defined role for these providers.
A research study in rural Nigeria found that PPMVs are a particularly important access point for basic health care services. They are usually members of the communities, and this makes them strategic influencers for people’s lifestyle and health choices.
The IntegratE Project
The IntegratE project, implemented by a consortium led by the Society for Family Health (SFH) with funding from MSD for Mothers and in partnership with the Bill & Melinda Gates Foundation has, since 2017, been working with the Federal Ministry of Health (FMoH) to broaden its task-shifting task-sharing (TSTS) policy. This is being done by piloting a system led by the Pharmacists Council of Nigeria (PCN), to test a task-shifting model in Lagos and Kaduna States with the view to scale up to other states. The project aimed to improve access and uptake of family planning services with the overall objective of improving contraceptive coverage.
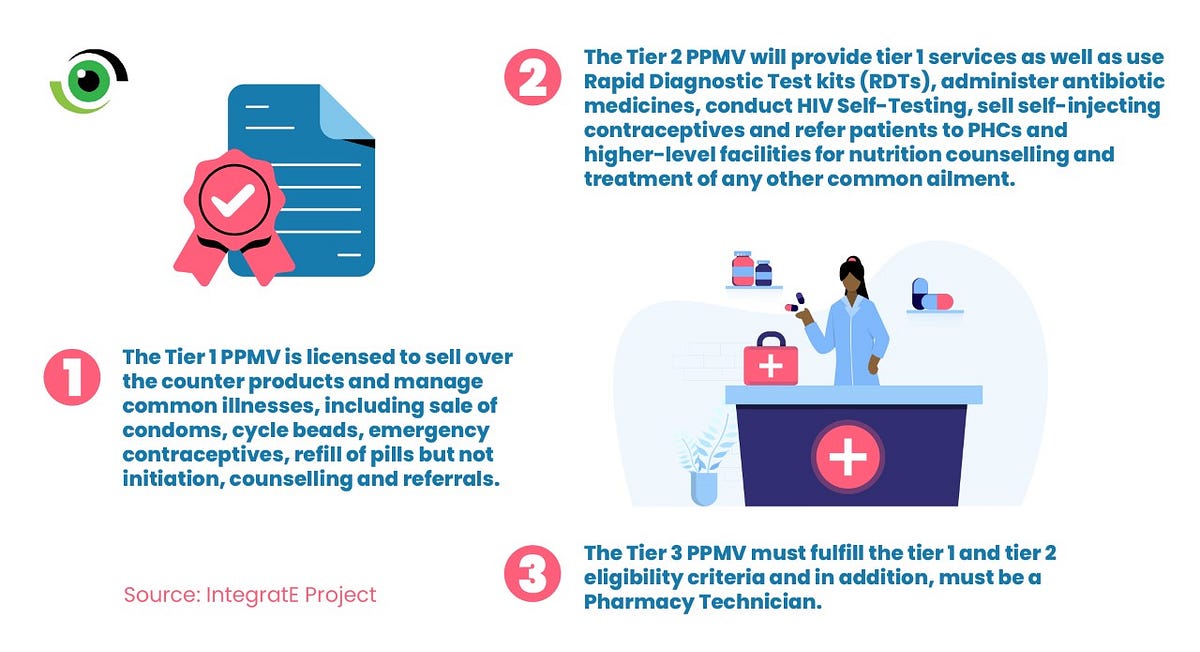
Between 2017 and 2021, IntegratE employed a 3-tier accreditation system that recognised the heterogeneity of PPMVs, presenting an opportunity to scale up basic health care services, especially in rural communities in line with the current task-shifting task-sharing policy. The project is a proof of concept that Community Pharmacists (CPs) and Patent and Proprietary Medicine Vendors (PPMVs) have the capacity to provide a wider range of family planning (FP) and primary health care (PHC) services than they are currently authorised by law to provide.
Breaking Down the 3-Tier Accreditation System
Commenting on the rationale for working with PPMVs, Emeka Okafor, Project Director, SFH, IntegratE project stated that, PPMVs are an important source of care for the poor as they are located close to rural communities, and are often the first source of care for hygiene and FP products and treatment of childhood illnesses in these communities.
An Insight into the IntegratE Project
Results from a knowledge retention survey conducted by the project revealed that CPs and PPMVs who received training on the expanded scope of FP services including FP counseling, injectable administration, and implant insertion/removal, retained this knowledge over time. Results from client exit interviews obtained from women who had received FP services from the trained CPs and PPMVs showed that clients reported close relationships with the IntegratE service providers. The women described the CPs and PPMVs they visited as ‘motherly’, ‘friendly’, ‘warm’, ‘caring’, ‘patient’, and ‘respectful’.


Zainab Aliyu, Registered Nurse/ Midwife (Tier 2 PPMV) in Kaduna said, “People are particular about the cost of the family planning commodity, and that has discouraged turnout. Despite that challenge, facilitators of the IntegratE project are putting in their best to change buy-in behaviour through regular social and behaviour change communication and advocacy”.
Benefits of Adopting a Tiered Accreditation Model for PPMVs
The IntegratE pilot project revealed that broadening the current task-shifting task-sharing model to include tiered PPMVs will help to improve access and the quality of FP and PHC services provided by CPs and PPMVs in rural, peri-urban, and hard-to-reach communities.

If trained and properly supervised, Tier 1 PPMVs, can provide balanced counselling services for family planning, refill of oral contraception pills and make referrals for other services. Tier 2 PPMVs can safely provide Injectables and implants as well as elect PHC services, especially in hard-to-reach and rural communities. CPs in Tier 2 and Tier 3 PPMVs can improve access and scale-up PHC services especially in underserved communities and will be vital in meeting global Universal Health Coverage (UHC) goals. CPs and PPMVs can be trained to routinely provide service delivery data which can be integrated into the National Health Management Information System NHMIS). This will provide the country with comprehensive data for evidence-based decision-making and planning.
Achieving an Inclusive, Impactful and Sustainable Family Planning Ecosystem
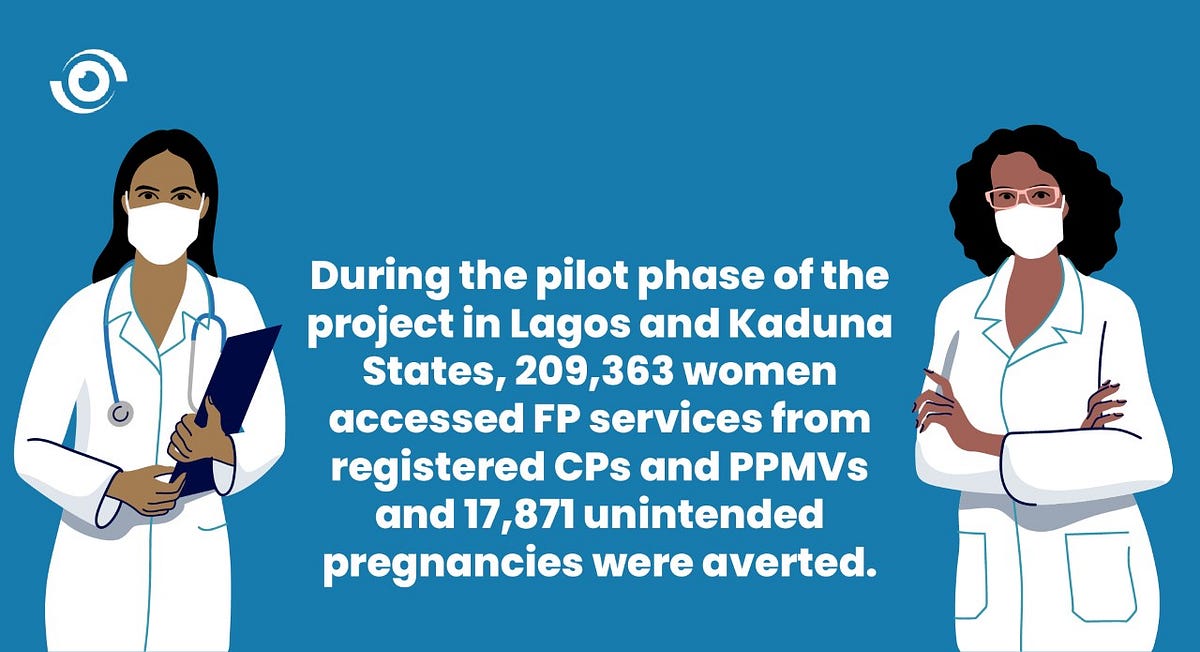
Ultimately, this pilot phase of the project has shown that improving access to family planning products and services and freeing up time for health care workers to focus on providing complex services allows for a more efficient family planning service value chain. This pilot has provided evidence of the integral role that the informal sector can play in increasing access to FP services, especially in rural underserved communities. These gains can be leveraged by scaling up the use of CPs and PPMVs in other states in Nigeria.


Through the Nigeria Family Planning Blueprint (2020–2024), the Federal Government has set a target to achieve Nigeria’s Modern Contraceptive Prevalence Rate (mCPR) of 27 percent by 2024. Public-private partnerships, a national plan for effective distribution of FP services and increased financing at national and state levels will help accelerate its implementation.
The existing TSTS for essential healthcare services policy must be revised to enable trained CPs and PPMVs in Nigeria to provide FP services to underserved communities. A revised TSTS policy, inclusive of CPs and health-trained PPMVs, has the potential to dramatically improve access to primary health care for Nigerians, especially underserved populations, and expand services and supplies through these retail channels in a way that ensures quality and sustainability.
The IntegratE project has provided a viable model for the accreditation and tiering of PPMVs to provide expanded FP services for underserved populations. The Pharmacists Council of Nigeria through the FMOH should push for national adoption of the model. This will enable state governments to design frameworks for its adoption, which will further spur the revision of the current TSTS policy on one hand and galvanise increased budgetary allocation to FP on the other hand. In February 2020, the Kebbi State Ministry of Health launched the state TSTS Policy for Essential Health Care Services, thus expanding access to FP services and commodities at the community level in the state.
To achieve the Federal Government target of 27 percent Modern Contraceptive Prevalence Rate (mCPR) by 2024, stakeholders at local, state and federal levels and the private sector must work together to effectively mobilise domestic resources to ensure that every pregnancy is planned and safe for the mother.