


Sunday Oko and Tzar Oluigbo (Lead writers)
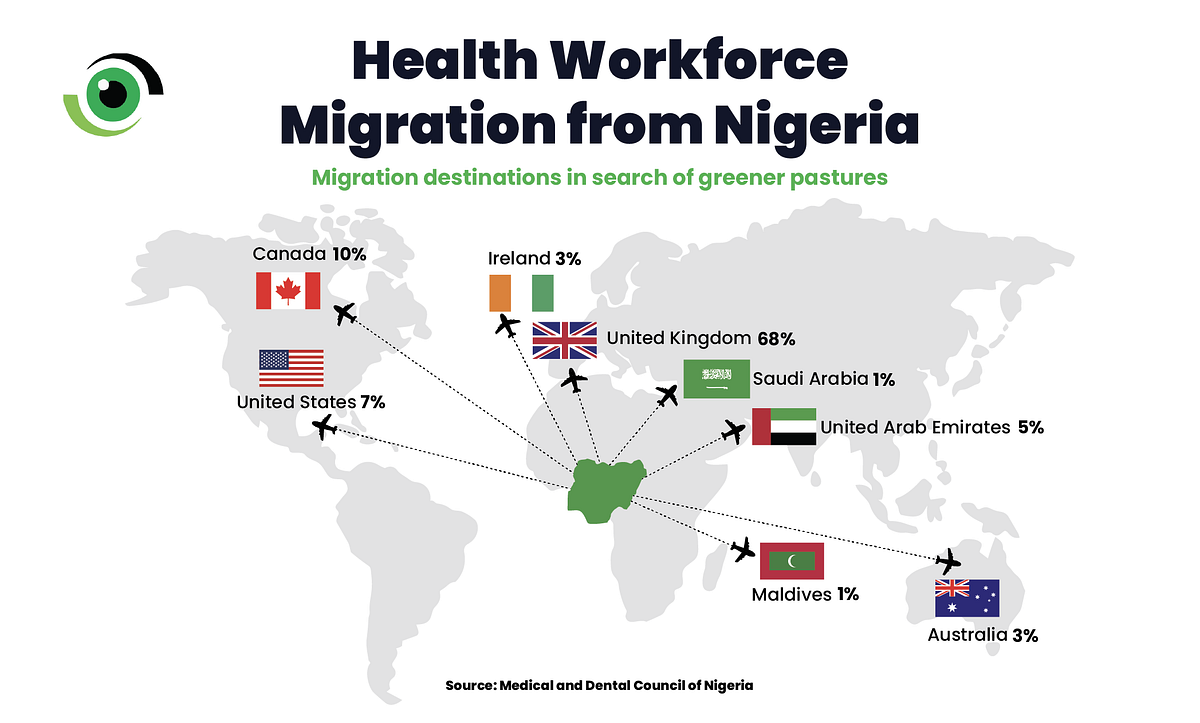
On 12 August 2024, the Federal Government of Nigeria approved the long-awaited National Policy on Health Workforce Migration. The policy was presented as a practical response to a growing and highly visible crisis, where requests for letters of good standing had become a replacement for accelerating outflows, including a documented peak of over 3,000 doctors seeking clearance in 2022. This occurred alongside steep increases across other cadres, even as Nigeria’s health worker density remained far below the thresholds associated with adequate coverage.


Rather than frame migration as an offence to be suppressed, the policy positioned it as a reality to be controlled, explicitly recognising freedom of movement and aligning Nigeria’s approach with the WHO Global Code on International Recruitment, while promising a shift from ad hoc reactions to managed migration backed by real-time data, clearer institutional accountability, and structured bilateral engagement with destination countries.
Nearly two years on, with the government publicly canvassing “ethical” and mutually beneficial arrangements with top destinations and early retention signals such as clinician housing interventions entering the public domain, the defining test is whether this policy has moved from a statement of intent to a funded, measurable reform that frontline teams can feel in safer working conditions, fairer incentives, and a more stable distribution of staff across the health system.


What the policy set out to do, and why it mattered
At its core, the National Policy on Health Workforce Migration commits to three complementary goals: to strengthen data and track movements, to improve retention, especially in underserved and rural areas, and to establish ethical, bilateral and whole-of-government processes for managed migration. It links explicitly to the WHO Global Code on International Recruitment and calls for investment in training capacity, career pathways, and incentives to retain clinicians in Nigeria. For a country reported to have lost 75,000 nurses between 2020 and 2025, these pillars are sensible; but only if they are financed and enforced through clear accountability.

The policy delivered an early outcome that many reforms need before anything else by changing the terms of the debate. Health worker migration was no longer treated as an unavoidable loss; it was reframed as a workforce issue that government, regulators, and other stakeholders must recognise, plan for, and manage. This shift in visibility was important. It created room for more structured engagement with professional regulators, training institutions, and international partners on shared responsibilities, data needs, and practical options.
The policy also pushed the system towards stronger evidence. Its emphasis on routine tracking through the National Health Workforce Registry, alongside coordinated reporting, encouraged pilot data exercises and initial assessments. Reliable information is essential for matching workforce supply to service needs. Early steps to standardise reporting were therefore useful, even if implementation remains uneven. Ultimately, the policy broadened what “retention” and “motivation” mean in practice. It acknowledged that incentives are not only financial. It highlighted career progression, rural hardship allowances, and training opportunities as part of a wider package. This was a meaningful shift away from earlier debates that focused narrowly on pay, and it better reflects how health workers make decisions about staying, moving, or returning.
Where the policy is falling short
A policy without budget lines and clear, time-bound deliverables will stall. Nearly two years on, many flagship proposals such as expanded training capacity, establishing Human Resource for Health (HRH) units at state level, and building interoperable registries, remain at pilot or planning stage. Without sustained financing and clear accountability, the policy risks becoming a well-intentioned document with limited practical effect. Health workers continue to cite heavy workloads, poor working conditions, and unclear career pathways as key push factors. A national policy is necessary, but it will not deliver results unless states adopt, adapt, and fund its measures. Implementation is already uneven across the country. This creates disjointed action that weakens overall impact and makes it harder to track progress, compare outcomes, and plan nationally.
The policy will only succeed if federal and state actors work in a coordinated way, with clear roles, shared targets, and practical support for implementation. Federal government should also use appropriate incentives to encourage state adoption, including technical assistance, aligned funding mechanisms, and performance-based accountability. The policy envisaged ethical bilateral agreements with destination countries and clearer regulation of recruitment agencies. Yet, formal bilateral arrangements and robust oversight of recruiters remain limited, creating space for unethical recruitment practices and poorly managed migration pathways.
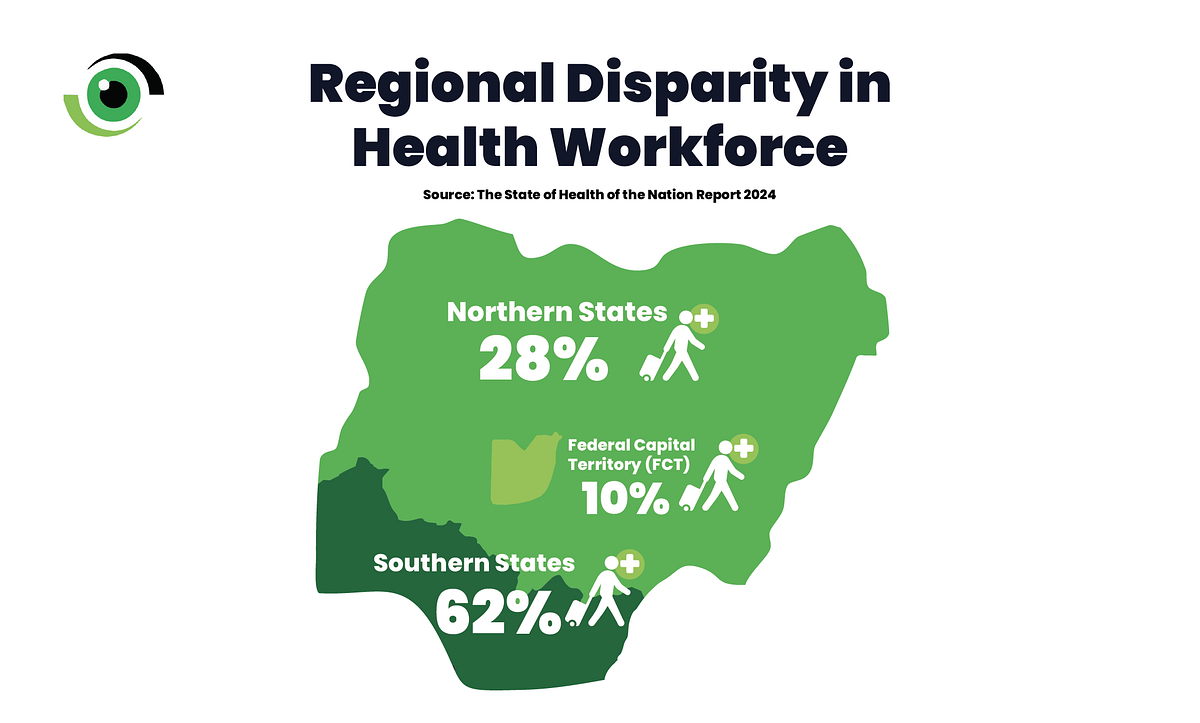
In October 2025, Nigeria launched a National Strategy for Nursing and Midwifery (2025–2030), to strengthen training, deployment, and performance of nurses and midwives. The strategy aligns with the emphasis of WHO’s Global Strategic Directions for Nursing and Midwifery (2021–2025) on retention and career development. At the same time, the Federal Ministry of Health’s State of Health of the Nation report highlights ongoing investment in health worker recruitment, while documenting persistent inequities. Nigeria’s health workforce is unevenly distributed. In many settings, more than 80% of health workers are concentrated in urban areas. Nationally, doctor density is 1 per 2,500 people, which is far below the thresholds associated with adequate coverage.
Practical recommendations that move from policy to delivery
To make the policy real and measurable, the government should adopt the following actions to resource implementation, test and scale what works, and embed accountability for results.
- Turn commitments into line-item budgets and milestones
Publish a costed implementation plan with clear milestones covering registry rollout, the number of additional training places, rural incentive packages to be tested, and the budget allocated to each activity. Donors and partners can then align support to measurable targets. - Scale pragmatic retention pilots fast
Fund rapid, state-level pilots that combine rural allowances, housing and transport support, continuing professional development, and safeguards against excessive working hours. Evaluate them against clear indicators such as vacancy rates, retention at 12–24 months, patient access, and scale what works. - Strengthen data systems and transparency
Complete the HRH registry rollout and agree interoperability standards across relevant systems. Require quarterly reporting on exits and verification requests from regulators and major employers and publish a minimum national dashboard to support transparency and accountability. - Negotiate ethical bilateral agreements that balance health worker mobility with health system needs
Prioritise provisions for training partnerships, short-term placements, fair recruitment standards, and pathways for return or circular migration. Move from policy intent to signed memoranda with clear implementation steps. - Centre the health worker voice
Involve professional associations, unions and frontline clinicians in implementation design, monitoring and review. Establish a structured feedback mechanism so policy decisions reflect on-the-ground realities in workload, safety, supervision and career progression.
Policy as a foundation, not a finish line
Nearly two years after its approval, Nigeria’s National Policy on Health Workforce Migration remains an important foundation that has helped reframe the national debate. However, foundations do not deliver services, people do. Unless the next phase prioritises funded implementation, state adoption, transparent data, and credible incentives that improve working conditions, migration will continue to erode service quality and access.
The policy’s promise can still be realised, but only if stakeholders convert words into budgets, pilots into scale, and data into decisions.