
Orode Doherty (Guest writer)
Traditional birth attendants (TBAs) remain a major source of maternity care in some Lagos communities, especially where women prioritise familiarity, proximity, flexible payment, and emotional support. Lagos State, through the Lagos State Traditional Medicine Board (LSTMB), oversees the registration and regulation of traditional medicine practitioners, including TBAs, and has publicly stated its intent to enforce registration and compliance measures.
Lagos State’s 2018 Maternal and Perinatal Death Surveillance and Response (MPDSR) summary shows maternal deaths concentrate around childbirth. Among reviewed deaths, 63% occurred during labour (11%) or postpartum (51%). The report also highlights gaps in documented antenatal care (ANC), where only 28% had ANC recorded, 36% had missing ANC information, and 46% had incomplete recording of the birth attendant type (unknown/not recorded). These are system warnings. Women are arriving late, risk is not being tracked, and accountability is weakened by missing data.
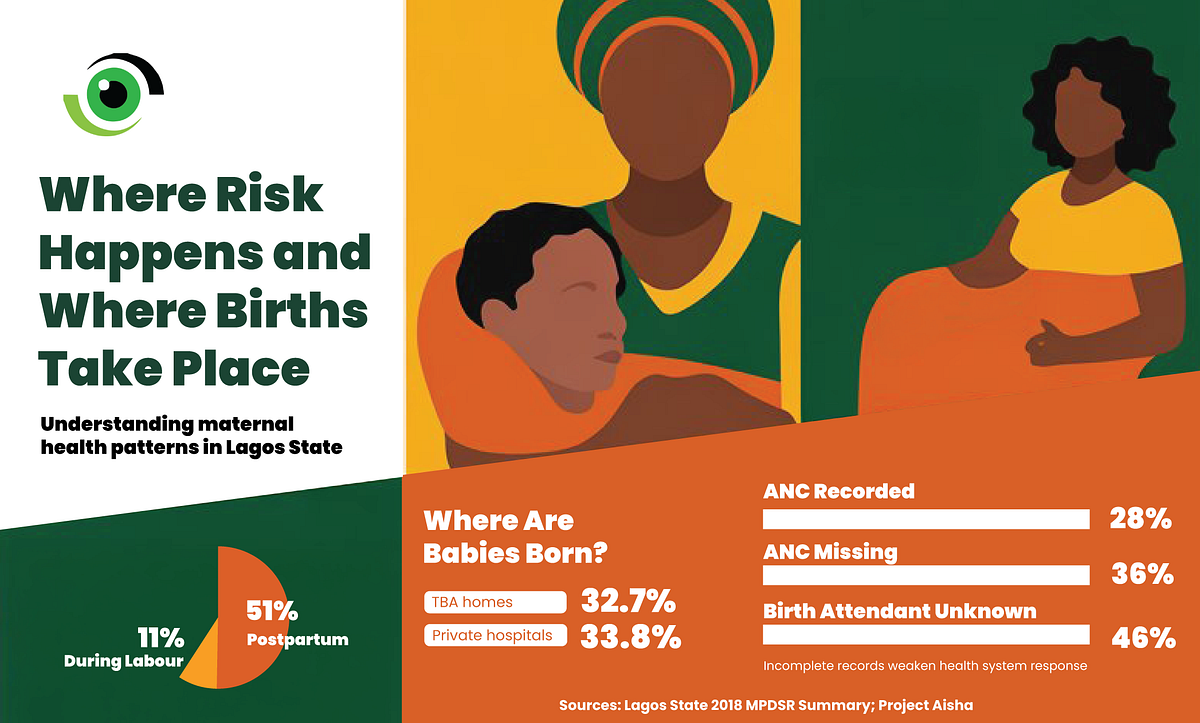
Project Aisha, funded by MSD for Mothers, launched a three-year intervention implemented in Lagos and Kaduna States to guide the overarching goal of reducing maternal mortality and obstetric complications by 20% from 2022 to 2025. To kick off implementation in Lagos State, Project Aisha conducted a baseline assessment in 23 communities across the Epe and Ifako-Ijaiye Local Government Areas (LGAs). In Project Aisha’s Lagos baseline, 32.7% of births occurred in TBA homes, alongside 33.8% in private hospitals, emphasising the need for safety efforts to address both informal and private providers, not only public facilities.
Why women choose TBAs and private providers, and what Lagos must learn
Project Aisha’s preliminary mapping also identified major oversight gaps in the two LGAs. In Epe, 44% of assessed TBA sites were unregistered, and 56% were not submitting service data at the time. In Ifako-Ijaiye, 12% were unregistered, and 29% were not submitting data. Poor registration and weak reporting reduce the state’s ability to see risk early and improve referrals. Qualitative findings suggest many women prefer skilled birth attendants, but some choose TBAs because of fear of medical interventions and negative provider attitudes, while household influencers such as husbands and mothers-in-law strongly shape decisions.
Among women who delivered in public facilities during the baseline, 12% reported verbal mistreatment and 6% reported physical handling such as slapping/pinching, reinforcing why respectful care is not “nice to have” but a trust and utilisation strategy. Rebuilding trust requires respectful maternity care, clear communication, consent, privacy, and non-abusive care because mistreatment reduces future care-seeking and weakens referral completion. Lagos already has community evidence of reported verbal and physical mistreatment in public facilities, and reducing this is part of risk reduction.
Regulating the private nurse-midwife practice
In Lagos, the Health Facility Monitoring and Accreditation Agency (HEFAMAA) requires public and private health facilities to register for ongoing monitoring, quality assurance, and health data reporting. HEFAMAA maintains distinct registration categories, including Private Nursing/Convalescent Homes and Maternity Centres, with different minimum staffing, safety, infection prevention, waste management, and referral expectations. This differentiation reflects childbirth’s higher clinical risk.
HEFAMAA’s Maternity Centre standards include more explicit expectations for emergency referral arrangements and maternity-specific competencies than the Nursing/Convalescent category. In contrast, nurse-midwives working within registered nursing or convalescent homes are generally required to refer expectant mothers to primary health centres (PHCs), hospitals, or accredited maternity homes for antenatal care and delivery — except in urgent situations, such as when the baby’s head is already crowning at the time of presentation.
Nurse-midwives as the default skilled provider closest to communities
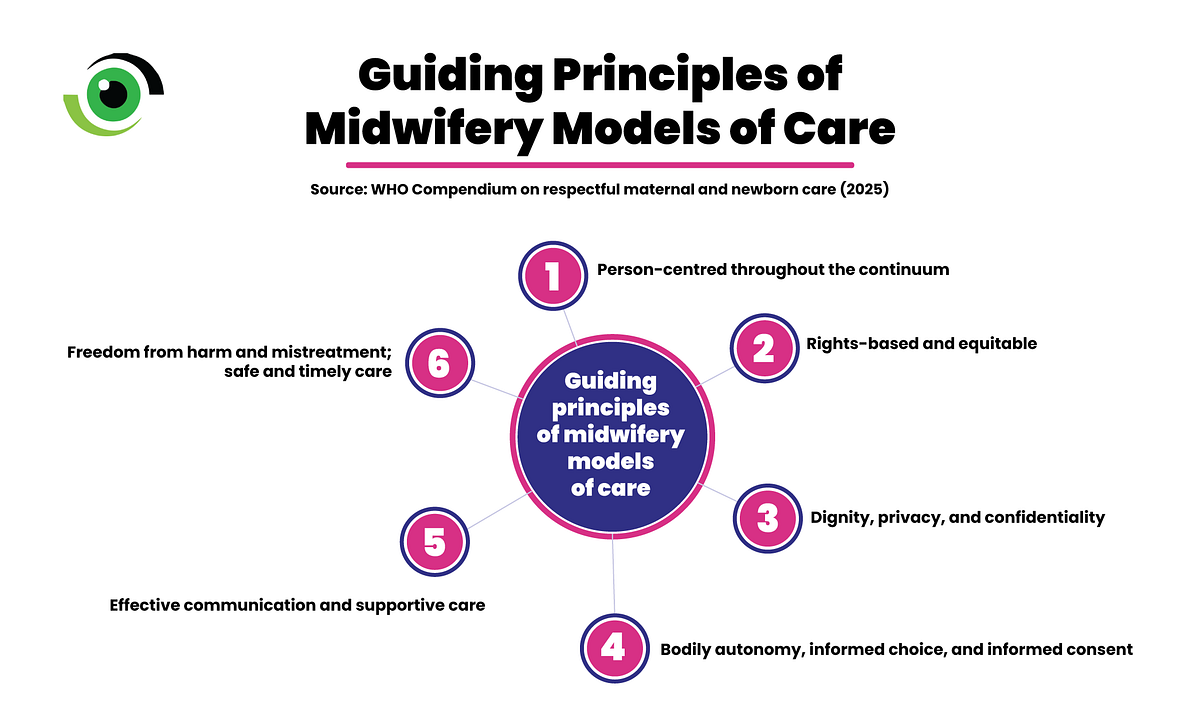
Project Aisha describes convening referral meetings between TBAs and public/private referral hospitals to develop referral forms and a system that tracks referral initiation through completion, an approach aimed at preventing deaths linked to late or incomplete referrals. Global evidence and policy guidance increasingly support midwife-led continuity of care and high-quality midwifery as core strategies for better maternal and newborn outcomes, especially when care is respectful and unnecessary interventions are avoided.

Image credit: Project Aisha
This model promotes continuity with a known midwife/team (where feasible), respectful, woman-centred care as a quality standard, and timely escalation and referral when complications arise, not anti-intervention, but right intervention at the right time. Project Aisha supports this shift by spotlighting the role of Registered Nurse-Midwives, expanding their visibility, and advocating for continuity of care in communities.
What Lagos should do now
The policy ask is to take these lessons beyond a project footprint and make them a standard. These three actions are specific, feasible, and measurable.
- Make it impossible to hide in the system. HEFAMAA should require every facility to display its registration category and approved services, including whether it can conduct deliveries, and then enforce these requirements strictly against facilities operating outside their scope. At the same time, Lagos State should intensify inspections and sanctions to stop quackery and illegal auxiliary nurse training/use, and run public campaigns that teach families how to verify licensed facilities and professionals.
- Turn maternity safety into a Lagos-wide baseline. Using HEFAMAA standards, require every registered maternity centre to meet and be audited against a minimum safety package comprising emergency readiness for eclampsia/hypertension and postpartum haemorrhage, partograph use, infection prevention, and documented referral agreements. Make respectful maternity care mandatory through training, supervision, and measurable indicators built into accreditation and mentorship.
- Build one functional system across public, private, and informal providers. Bring TBAs and all delivery points into registration and routine reporting, so MPDSR becomes a real prevention tool rather than just paperwork. Treat referral completion as the performance standard, track referrals from initiation to arrival, care received, and feedback returned, and hold regular LGA review meetings.
Many women deliver outside public facilities. Lagos State’s safest path is not to wish TBAs away or to ignore private practice. It is to make regulated, high-quality midwife-led care the default, strengthen respectful care, enforce against quackery, and use insurance and accreditation to shift demand towards safer providers. If Lagos wants no mothers to die giving life, it must back the providers closest to women with rules, skills, accountability, and financing that match the risk.