


Chidinma Peace Ahunam and Chisom Obi-Jeff (Guest writers)
In Nigeria, many children miss routine immunisation not because they are “hard to find”, but because services do not consistently reach them. In 2023, about 2.1 million children missed key routine doses, and in 2024, only 39% of children aged 12–23 months were recorded as fully immunised. This gap is long-standing, but the COVID-19 period worsened it by disrupting outreach, supervision, supply chains, and caregiver demand, leaving more children zero-dose or under-immunised.
In April 2023, the World Health Organization (WHO), UNICEF, Gavi, and partners launched the Big Catch-Up (BCU) to help countries restore and expand routine immunisation after COVID-19 disruptions. Nigeria translated this momentum into its Zero-Dose Immunisation Recovery Plan (2023–2028), with targets to reduce zero-dose numbers by 30% by 2025 and 50% by 2028. But the real test was not whether Nigeria could run another time-bound drive. It was whether catch-up could become a routine, funded, and accountable function of primary health care, able to reach children who miss doses.

A case study from Bauchi and Rivers States
The Alliance for Health Policy and Systems Research (HPSR), working with WHO’s Department of Immunisation, Vaccines and Biologicals, commissioned Brooks Insights and the Health Policy Research Group (HPRG) to examine BCU implementation in Bauchi and Rivers States.
The study set out to:
- document how catch-up activities were planned, delivered, and monitored;
- assess practical options for embedding catch-up within routine immunisation and Primary Health Care (PHC); and
- identify why under-immunisation persists even when intensified efforts are in place.
Between July and November 2025, the team combined routine monitoring data with fieldwork in both states, surveys of 750 caregivers and 180 health workers, observation of 47 vaccination sessions, 77 key informant interviews, and 21 focus group discussions. Quantitative findings were summarised descriptively, and qualitative data were analysed thematically, with triangulation across sources.
What worked in planning, implementation, and monitoring
The BCU demonstrated that reaching missed children is feasible, achieving 70% coverage (Penta2) in Bauchi State and 75% (Penta3) in Rivers State across the three rounds from December 2024 to April 2025. Planning largely used existing immunisation governance structures and multi-stakeholder coordination across government, partners, and communities, which supported shared ownership and clearer roles.
Microplans, strengthened by geospatial mapping and community input, helped identify zero-dose settlements and allocate teams and resources more realistically. Vaccine supply planning, forecasting, allocation by facility need, and last-mile distribution aligned with cold-chain capacity, reducing missed opportunities due to stockouts. Remarkably, these choices kept catch-up connected to state systems rather than creating a parallel structure.

The implementation directly addressed social, cultural, and access barriers. Community groups supported door-to-door mobilisation, while traditional and religious leaders participated in microplanning, supervision, and community dialogues. In Bauchi State, the State Emirate Council Committee on Health strengthened trust, and peer networks such as Mama-to-Mama and Fathers-for-Good-Health helped make immunisation a shared norm. In Rivers State, ward development committees (WDCs) led community dialogues. Trust came not from posters and jingles alone, but from familiar voices, credible messengers, and respectful engagement.
A mixed delivery model, fixed sessions, outreach, and mobile teams helped reach different groups of missed children. Adjusted clinic schedules and early-morning outreach during farming seasons improved access, while phone reminders and community dialogues helped address low salience, competing priorities, and missed appointments.
In Bauchi State, service delivery adapted to mobility. With 13 of 20 LGAs contributing a large share of missed children, teams took services to families rather than waiting for families to attend facilities. Vaccination days were aligned with nomadic movement patterns, and mobile teams reached schools, markets, motor parks, transit routes, and border communities. In Rivers State, service delivery adapted to the riverine terrain. Riverine communities accessible only by water were reached by boat, making “riverine outreach” a practical routine option, but one that requires higher recurrent costs (boats, fuel, safety equipment) and tailored logistics.
Adaptation was supported by rapid monitoring and feedback loops. Daily review meetings enabled teams to identify bottlenecks quickly and adjust plans. Digital data tools such as Google Sheets and Open Data Kit (ODK) improved visibility, while ward-level validation before uploading to the District Health Information Software (DHIS2) strengthened data quality. Standardised supervision checklists helped maintain implementation standards. However, operational success did not erase the deep-rooted barriers that continue to leave some children unreached.
Why zero-dose and under-immunisation persists
Even with intensified delivery, 54–86% of children aged 24–59 months remained unreached. Health workers most often cited caregiver concerns and low confidence (79–95%), vaccination hours that did not fit work and household schedules (42–60%), and distance or transport constraints (33–53%). Using the WHO/UNICEF Behavioural and Social Drivers (BeSD) of vaccination framework, the constraints clustered across four connected domains:

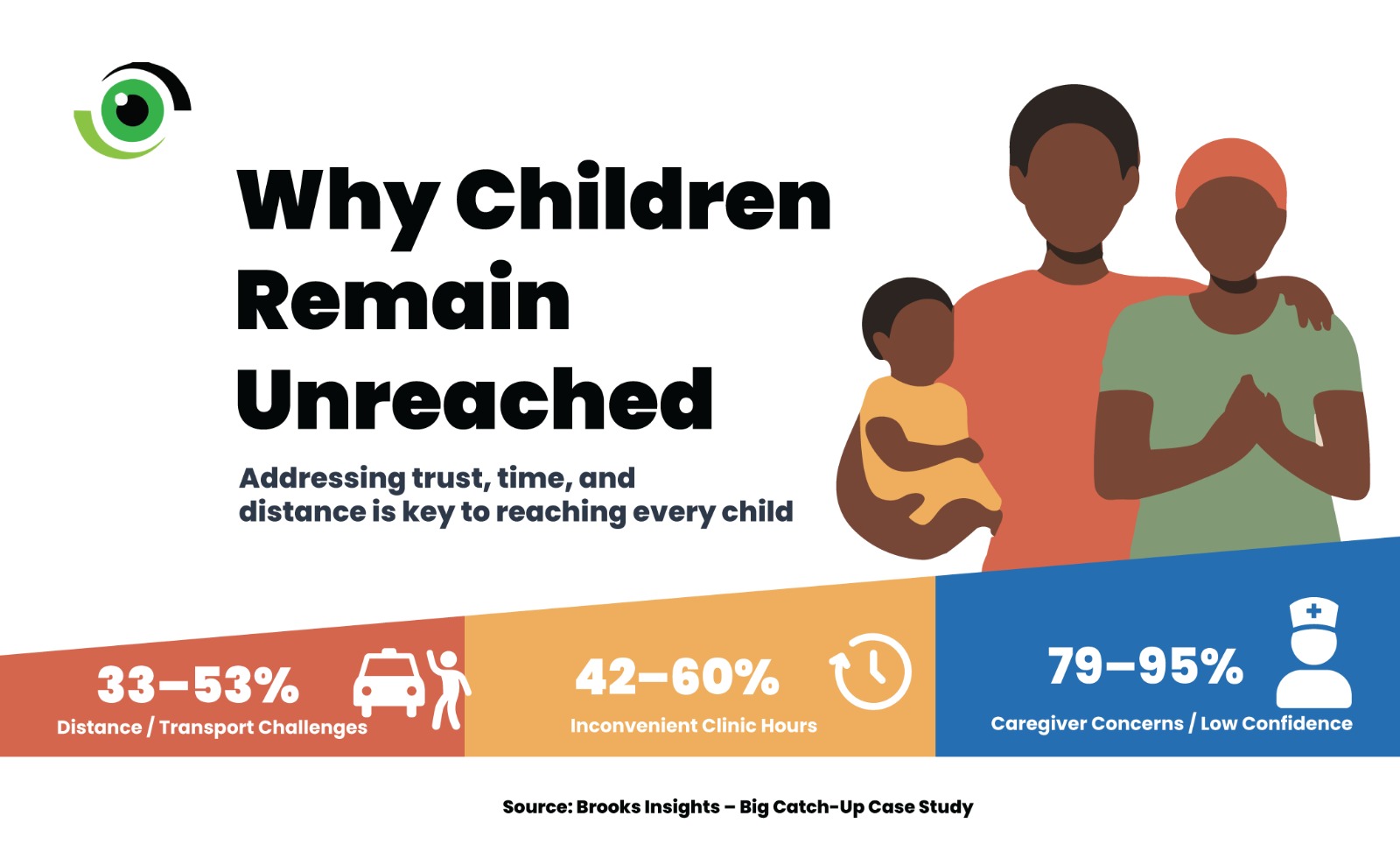
Image credit: Nigeria Health Watch
- Thinking and feeling: knowledge gaps, misinformation (including population-control narratives), fear of adverse events, forgetfulness, and distrust linked to weak service experience.
- Social processes: influence of traditional norms, gender dynamics where fathers may hold decision authority, extended family pressure, religious discouragement, and community conflict or displacement.
- Motivation and trust: low perceived benefit when services feel extractive, vaccination is pursued, but other priority needs (treatment, commodities, respectful care) are not addressed.
- Practical access: distance and transport cost (especially in riverine areas), stockouts and missed opportunities, inconvenient vaccination times, workforce gaps and poor provider attitude, difficult terrain, and inadequate cold-chain equipment.
These overlapping barriers show why routine immunisation, as currently organised and funded, cannot close the gap alone. Without improvements in service design, workforce support, sustained funding, supply reliability, and community accountability, Nigeria risks repeating catch-up cycles rather than preventing children from becoming zero-dose in the first place.
Catch-up works when it is treated as a system function
The BCU showed that missed children can be reached when coordination, logistics, supervision, and community engagement are adequately resourced. Signals of government ownership, such as counterpart funding in Bauchi State and inclusion in state work plans in both states, suggest growing momentum. Yet gains remain fragile where there is no formal policy direction, no dedicated budget line, unclear accountability for delivery, and no routine reporting framework that includes older catch-up age groups.
Catch-up becomes sustainable only when it is institutionalised, that is, treated as a routine PHC responsibility with policy authority, funding, workforce, and measurement. Practically, this requires:
- Policy and guidance: a clear national and state directive that defines catch-up as a routine function, with minimum standards for session frequency, outreach, and follow-up.
- Service design integration: embedding catch-up into routine delivery and structured intensification approaches (including periodic intensification of routine immunisation) without reverting to parallel campaign systems.
- Dedicated operational financing: ring-fenced budgets for outreach, transport, supportive supervision, and cold-chain running costs, released on time and tracked.
- Routine data and accountability: updating DHIS2 reporting to capture 12–59 months catch-up, with age-disaggregation and clear indicators for zero-dose identification and conversion.
- Workforce and community platforms: shifting from ad-hoc volunteer reliance to paid, supervised community health roles with defined responsibilities for mobilisation, defaulter tracing, and community feedback.
Institutionalisation must also reflect local realities. In riverine areas, boats and fuel are not “extras”; they are routine delivery costs. In nomadic settings, seasonal mobility should shape microplans, session timing, and team placement. A one-size-fits-all model will continue to miss the children that routine services repeatedly fail to reach.
This piece draws on validated findings from the BCU case study, led by Chisom Obi-Jeff from Brooks Insights and Prof. BSC Uzochukwu from HPRG (July-November 2025), supported by national and state immunisation stakeholders, and documented in the BCU policy brief.