


Yasir Jamal Bakare and Vivianne Ihekweazu (Lead writers)
The preliminary figures from the Organisation for Economic Co-operation and Development (OECD) report landed like a final verdict. Official development assistance from the world’s wealthiest nations fell by 23.1% in real terms in 2025, the largest annual decline in the entire history of recorded foreign aid.
This is not a temporary dip or fluctuation caused by a bad year but reflects a long-term structural shift. No country on the African continent feels its effects more than Nigeria. For years, health financing advocates have warned that building a health system on donor generosity is a gamble, and not a strategy for a country like Nigeria with its growing population.
The OECD’s preliminary 2025 ODA data has now supported that argument. This data now raises an important question: why has a country that once positioned itself as the largest economy on the continent remained so reliant on foreign aid to finance its health sector?
A structural shift in global health financing
This is a crisis that stems from deliberate political decisions made in the world’s most powerful capitals. Official Development Assistance (ODA) fell by 6.1% in 2024 and then by 23.1% in 2025, driven by mounting political and fiscal reprioritisation, bringing it to 4.2% below 2019 levels.
The United States decreased its foreign aid by 56.9% in 2025, the largest decline by any donor country in history. This was caused by the dismantling of the U.S. Agency for International Development (USAID) and by a wider effort to cut government spending, which accounted for three-quarters of the global decline in ODA in 2025 alone.

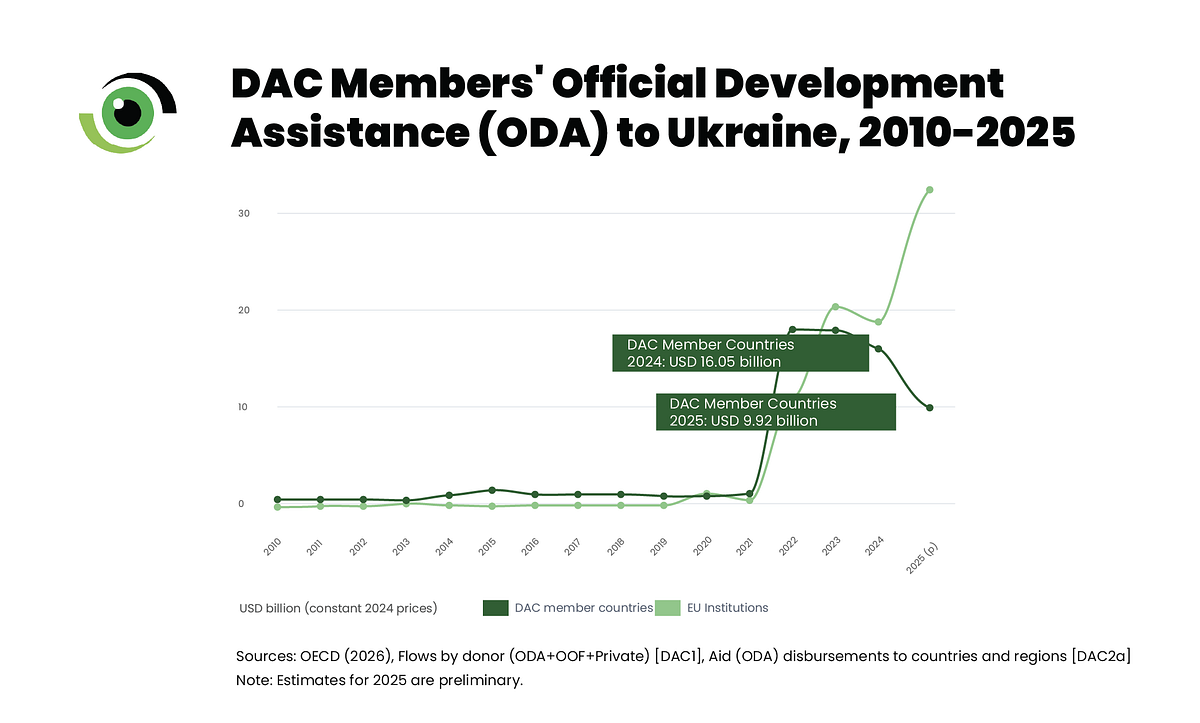
Germany, the United States, the United Kingdom, Japan and France accounted for 95.7% of the total decline, the first time in recorded history that all five of the highest donors have simultaneously reduced their ODA. The OECD projects a further 5.8% decline in ODA in 2026, with aid remaining 6.6% below 2025 levels through 2028. The era of aid flowing at the volumes Nigeria has relied on is over, with little indication that those levels will return.
The true cost for Nigeria: More than numbers
Rukayya (not her real name), a 26-year-old mother of three in Gombe State, does not know what “ODA” means. She only knows that the clinic near her home, where her children received immunisations and were screened for malnutrition, became unreliable in 2025.
She now travels further to another health facility and waits longer to be seen by a health worker. This has increased her out-of-pocket costs, which she cannot afford, forcing her to make difficult choices about when to seek care. Her experience is the human face of declining health funding, beyond what the statistics alone can show.
Nigeria alone has lost over $600 million in health funding, accounting for more than one-fifth of its annual health budget. As a result, health programmes have come under pressure, placing additional stress on already fragile health system infrastructure.
The human toll is similarly easy to measure. Reductions in USAID funding across six West and Central African countries, including Nigeria, are expected to increase maternal mortality rates by around 45% among populations in humanitarian need, with Nigeria experiencing the largest absolute increase of over 300 additional deaths in a single year. These are not projections about a distant future; they describe disruption already unfolding in real time across health systems.
If you cannot get aid, can you borrow? Not so easily
Some may ask, if donors are pulling back, why not simply borrow more? The answer is sobering. New research from ONE Data, supported by The Rockefeller Foundation, shows that the average cost of borrowing for African countries increased by 91% between 2020 and 2024, rising from 2.7% to 5.1% over just five years. This surge in borrowing costs affects every source of finance.
The chart from ONE Data visually shows the full story. Every creditor line shows an upward trend. The World Bank’s International Bank for Reconstruction and Development (IBRD) rates increased from 1.4% to 5.2%, a rise of over 270% in five years. China’s lending rates for Africa rose from 2.5% to 5.7%. Bondholders now charge 8.2%.
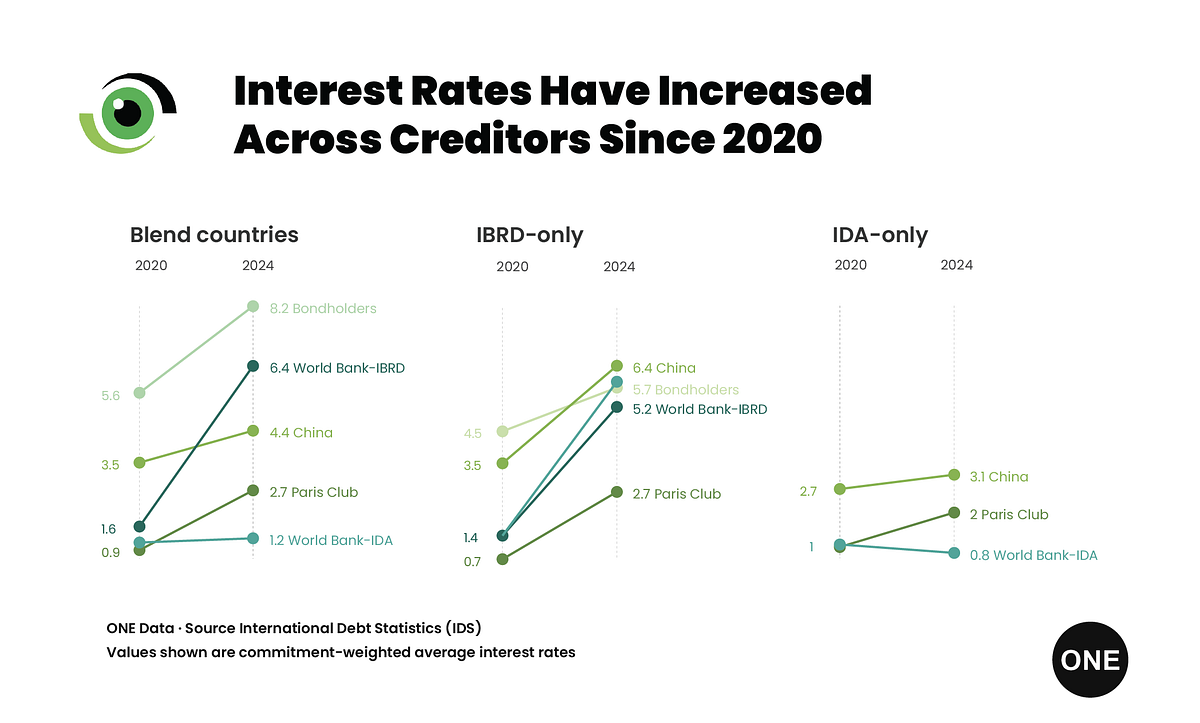
Countries like Nigeria find themselves in what researchers call the “squeezed middle.” They are not poor enough to access the World Bank’s most concessional International Development Association (IDA) rates (often with zero to low interest rates), but not wealthy enough to easily borrow on international bond markets. This is an exposed and uncomfortable position, especially now.
And the situation is set to worsen. As David McNair, Executive Director at ONE Data, noted in the report: “The cost of borrowing for African countries rose 91% between 2020 and 2024. These high costs were already putting a significant squeeze on investments in human development as countries struggle to service expensive debt. Now, with the Iran war threatening to increase energy and food prices significantly, the space countries’ ability to weather this crisis is severely limited.”
Meanwhile, in 2025, African countries were projected to spend about $81 billion on debt repayments, a figure that exceeds expected foreign funding inflows. Nigeria is paying more to service old debt than it can attract in new aid; this points to a tightening fiscal constraint that goes beyond a typical development financing gap.
Nigeria’s response: Moving in the right direction, but not far enough
Nigerian policymakers responded to the suspension of USAID-funded health programmes with a supplementary health budget of $200 million, directed towards immunisation and epidemic response. The Coordinating Minister of Health and Social Welfare, Professor Muhammad Ali Pate, reflected this position when he stated, “The responsibility to provide healthcare for our citizens ultimately rests on us.”


The 2026 Federal Budget allocates N2.149 trillion to the Federal Ministry of Health and Social Welfare, accounting for 3.67% of the proposed N58.47 trillion expenditure and a decline from the N2.83 trillion allocation in 2025.
When all health-related provisions across other ministries and agencies are combined, the total health allocation amounts to N2.915 trillion, approximately 4.98% of the overall budget. This falls short of the 15%commitment made by African heads of state under the Abuja Declaration, with Nigeria currently allocating roughly one-third of that target. Although the health allocation appears higher in absolute terms than in previous years, it still represents a relatively small share of total federal expenditure.
Domestic revenue generation is the solution
Nigeria must fund its own health system more decisively using domestically generated resources, particularly by making better use of the tools that already exist but remain underutilised. Health taxes on tobacco, alcohol, and sugary drinks are provided for under the Nigeria Healthcare Financing Policy, yet their proceeds are not consistently earmarked for health.
The 2026 budget does not clarify how these revenues will be used. At the same time, mandatory health insurance, which could generate an estimated N6 trillion in annual premiums, is not matched by adequate provisions for awareness or enforcement in the 2026 budget.
Other African governments are progressing more rapidly. Ghana removed the cap on its National Health Insurance Levy, ensuring all proceeds go directly to health. Ethiopia introduced a new workers’ tax to replace USAID-funded programmes. Nigeria signed the Accra Health Sovereignty declaration. Its budget should reflect that commitment.
More money is not enough without accountability
Over the past four years, Nigeria’s health capital budget was utilised at an average of just 31.49% of the approved amount and an appropriation of 37.86%. Out of N1.406 trillion appropriated from 2021 to 2024, only N532 billion was released, and only N381 billion was spent.
The problem of releasing and using funds is just as harmful as underfunding. Support for increased budgets must be combined with proper oversight of actual disbursements. What matters is that the budget appears much smaller if most of it never reaches a health facility.
As William Asiko, the Senior Vice President and Head of the Africa Regional Office at The Rockefeller Foundation, stated, “When the cost of borrowing rises this fast, countries don’t just lose access to capital; they lose the ability to invest in their future.”
The decline in global aid should end any remaining illusion that Nigeria can outsource the survival of its health system. What is happening is a lasting shift in the global financing landscape, not a short-term funding shock that Nigeria must respond to.
“Never before in history have we seen such a sudden, dramatic decline in ODA from one year to the next,” said Carsten Staur, chair of the OECD’s Development Assistance Committee. “Never.”
This is the moment for the federal government to make clear fiscal choices, including increasing health funding and ensuring timely fund releases. Recent experience with fund releases has been discouraging. When the Honourable Coordinating Minister of Health and Social Welfare announced that a mere ₦36 million out of a ₦218 billion capital allocation for 2025 had been released, there was the expected outcry.
Further avenues to strengthen health financing include putting into effect mandatory health insurance and earmarking health taxes, with the funds channelled into service delivery. Nigeria, now more than ever, needs sustained health financing that scales to address the country’s health challenges and improve health outcomes, because this time round, no one is coming to our rescue.
As we enter an election period, it is time for Nigerians to ask: how will their health be funded