
Oladimeji Solomon Yemi and Safiya Shuaibu Isa (Lead writers)
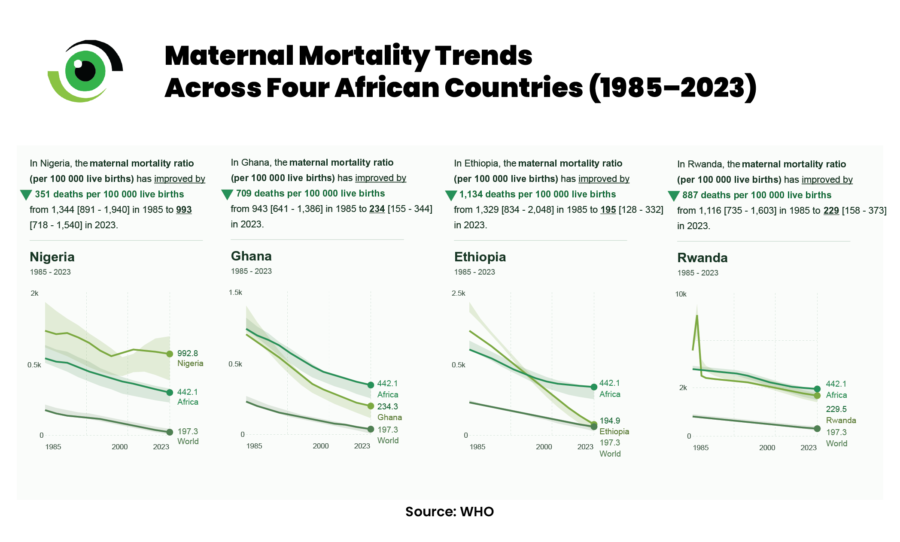
Nigeria remains one of the countries with the highest number of maternal deaths globally, with a maternal mortality rate of 993 deaths per 100,000 live births. While maternal mortality has declined globally over the past two decades, Nigeria has lagged behind both regional and global trends. In contrast, countries such as Ghana, Ethiopia, and Rwanda, which once faced similar challenges, have made significant gains by investing in skilled birth attendance, strengthening primary health care, and improving referral systems.
In Nigeria, community-informed maternal death reviews carried out between May 2019 and May 2020 show that many maternal deaths occurred outside formal health facilities, including at home, in traditional birth attendant (TBA) settings, or in faith-based centres. Even when facility-based deaths occur, they are often the result of delayed referrals rather than isolated failures of clinical care. Communities point to poor access to quality services, shortages of skilled health workers, weak referral systems, long distances to care, and persistent cultural beliefs as key drivers of maternal mortality.
Why are women dying while giving birth in Nigeria?
Nigeria’s slower progress cannot be attributed solely to poverty or population size. Several countries with comparable or lower gross domestic product (GDP) per capita have recorded steeper declines in maternal mortality. The divergence reflects differences in how health systems are organised, financed, and held accountable, particularly in aligning resources with skilled birth attendance coverage and emergency obstetric care. Nigeria has yet to apply this alignment consistently at scale.
The medical causes of maternal death in Nigeria are well known and largely preventable. Postpartum haemorrhage (PPH) remains the leading cause. Each year, about 14 million women experience PPH globally, requiring rapid access to uterotonics, blood transfusions, and skilled emergency care, services that are often unavailable or reached too late. Hypertensive disorders, including pre-eclampsia also contribute significantly, despite being detectable and manageable through routine antenatal care and timely referral. Sepsis, prolonged or obstructed labour, and complications from unsafe abortion further increases the risk, particularly where surgical capacity and postnatal care are limited.
However, maternal deaths rarely result from a single clinical event. Community death reviews consistently show cascading delays, including delayed recognition of danger signs, delayed decision-making, delayed transport, and delayed treatment upon arrival. These delays reflect systemic weaknesses, not medical uncertainty. Women are dying not because complications are untreatable, but because health systems fail to respond in time. Patterns of service utilisation reveal a critical disconnect in Nigeria’s maternal health system: while antenatal care attendance is relatively high, facility-based delivery and skilled birth attendance remain significantly lower.
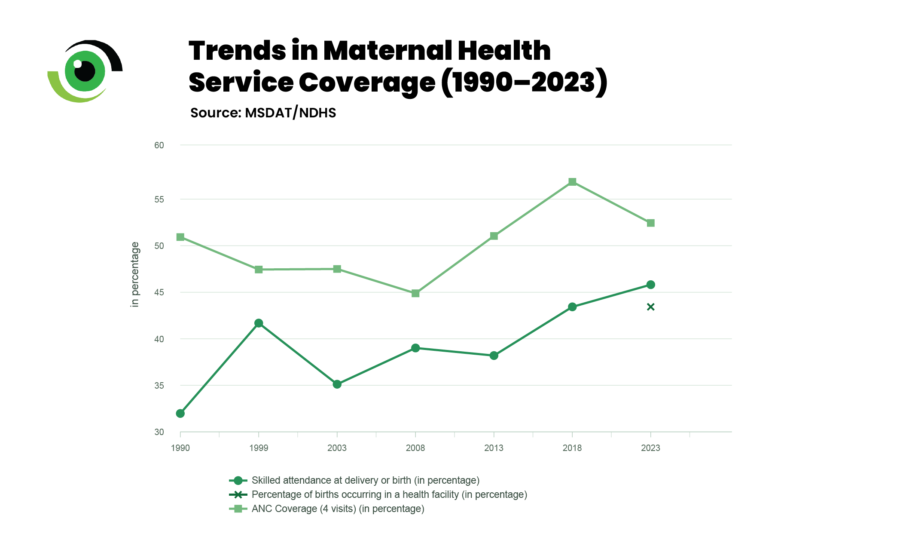
The 2024 Nigeria Demographic and Health Survey shows that 52.4% of women completed at least four antenatal visits, yet only 43.3% of births occurred in a health facility, and 45.7% were attended by skilled providers. This means that nearly one in two women who engage with the health system during pregnancy do not ultimately deliver under conditions equipped to manage obstetric emergencies. This gap is strongly shaped by geography and socioeconomic status. Women in urban and southern states are far more likely to deliver in facilities than those in rural and northern communities. In many high-burden states, most births still occur outside formal health facilities.
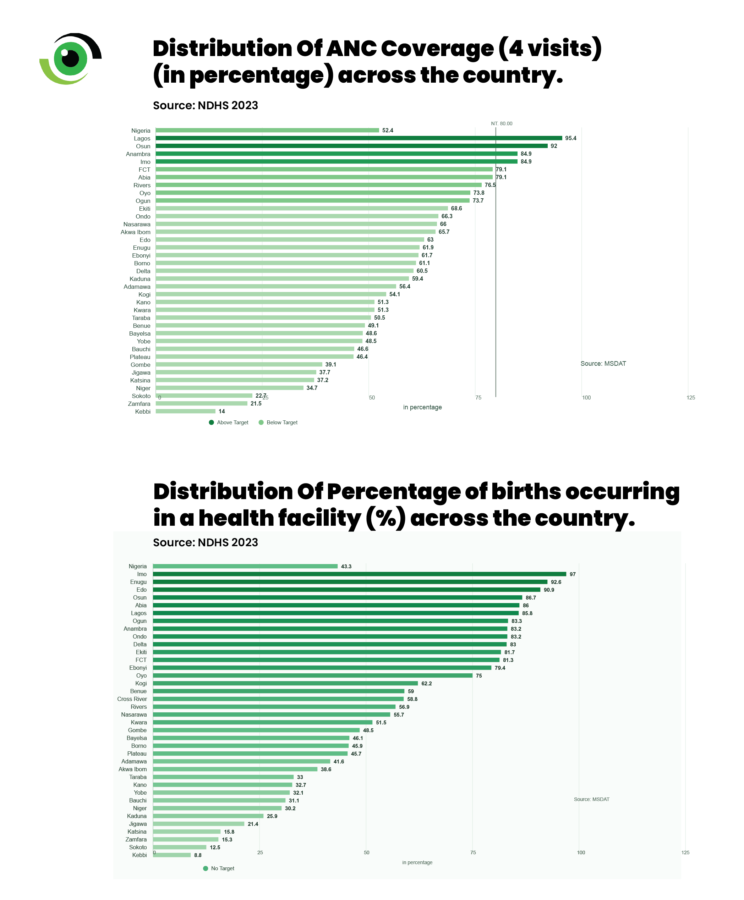
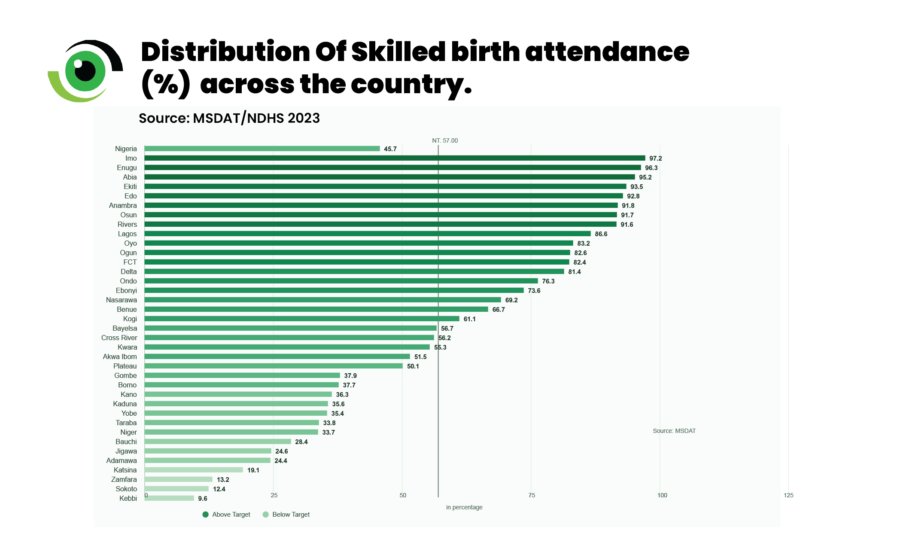
The disparities are stark. In Lagos (95.4%), Osun (92%), and Anambra (84.9%), ANC coverage is high. In contrast, in Kebbi (14%), Zamfara (21.5%), and Sokoto (22.7%), fewer than a quarter of women complete four visits. The same divide is reflected in delivery outcomes: while facility births exceed 90% in states such as Imo and Enugu, they fall below 15% in Kebbi, Sokoto, and Zamfara. Skilled birth attendance follows a similar pattern, exceeding 90% in parts of the south but remaining below 10–15% in several northwestern states.
Physical barriers such as distance, transport, and cost remain significant. Equally important are experiential barriers. Perceptions of poor treatment, neglect, or disrespect discourage the use of facilities, while traditional birth attendants are often seen as more accessible and supportive. Community death reviews reinforce this pattern. Many women who die either never begin their care journey in formal facilities or arrive only after prolonged delays. In such cases, deaths in facilities are not isolated clinical failures, but the endpoint of systemic breakdown.
What the Nigerian government is doing and why MAMII exists
Nigeria has introduced a range of policies to reduce maternal mortality, including efforts to expand skilled birth attendance, promote antenatal care, and institutionalise Maternal and Perinatal Death Surveillance and Response (MPDSR). More recently, maternal health has been prioritised within broader reforms under the Nigeria Health Sector Renewal Investment Initiative (NSRII), supported by mechanisms such as the Basic Health Care Provision Fund.
Yet a persistent limitation has been an incomplete picture of what is happening on the ground. MPDSR implementation in many settings has focused primarily on facility-based maternal deaths, leaving community-based deaths underreported. The Maternal Mortality Reduction Innovation Initiative (MAMII) was established to address these gaps by focusing on high-burden local government areas (LGAs) and facilities to improve prioritisation and response. By improving surveillance and linking data to targeted interventions, the initiative seeks to ensure that evidence informs decision-making rather than merely generating additional estimates.
Has MAMII reduced maternal deaths yet?
Recent reporting ahead of the 2025 Joint Annual Review indicates a 17% reduction in maternal deaths and a 12% decline in newborn deaths across 172 high-burden LGAs targeted under MAMII. These figures are encouraging, particularly in a context where progress has historically been slow. However, the reductions are programme-specific and largely reflect facility-based data. As noted in WHO guidance, MPDSR surveillance systems often capture facility deaths more consistently than community deaths, which can influence how trends are interpreted.
A significant proportion of maternal deaths in Nigeria occur outside formal health facilities or follow delayed referral. This means that data should be interpreted with caution. While MAMII appears to be improving the conditions for impact, whether these gains translate into a nationwide decline will depend on how effectively its core pillars, particularly around emergency obstetric and newborn care, are implemented and scaled.
What the data is really saying
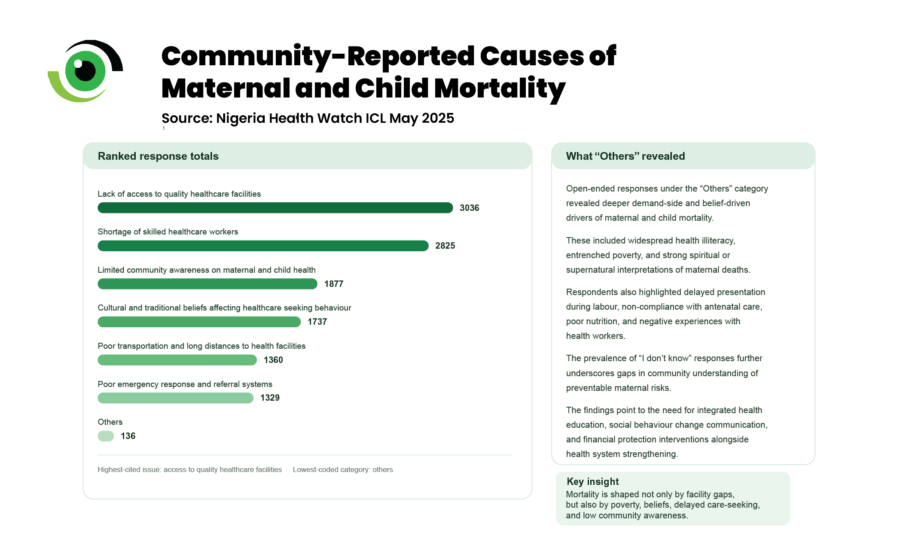
Findings from Nigeria Health Watch’s Integrated Community Listening (ICL) in May 2025 across Borno, Cross River, Ebonyi, Kano, Lagos, and Niger States showed that communities consistently attribute maternal deaths to poor access to quality facilities, shortages of skilled health workers, weak referral systems, and long distances to care. These insights align with earlier community death reviews, which found that many maternal deaths occur outside facilities or follow delayed referral, reinforcing that the underlying structural drivers remain unchanged.
Delays remain central. Even when danger signs are recognised, transport is unreliable, referral pathways are fragmented, and emergency capacity is inconsistent. These are patterns consistent with the Three Delays Model framework. At the same time, limited awareness and deeply rooted beliefs shape care-seeking behaviour. Evidence also shows that experiences of disrespect, neglect, or abuse during childbirth can deter women from using health facilities for delivery, contributing to continued reliance on non-skilled attendants.
This challenges narratives that place responsibility on women’s choices rather than on the health system’s ability to provide respectful, quality care. Maternal deaths tend to cluster where systems fail, where facilities lack emergency obstetric readiness, referral chains break down, and trust in formal care is weak. The persistence of these patterns suggests that the crisis is not a moving target. The solutions are known; failure lies in implementation and accountability.
What needs to change to end maternal mortality in Nigeria
Skilled birth attendance must be treated as a minimum standard, particularly in high-burden LGAs. Evidence consistently shows that having skilled healthcare workers present at birth is one of the most effective ways to prevent maternal deaths. High antenatal coverage alone is insufficient if women ultimately deliver without access to trained providers capable of managing complications.
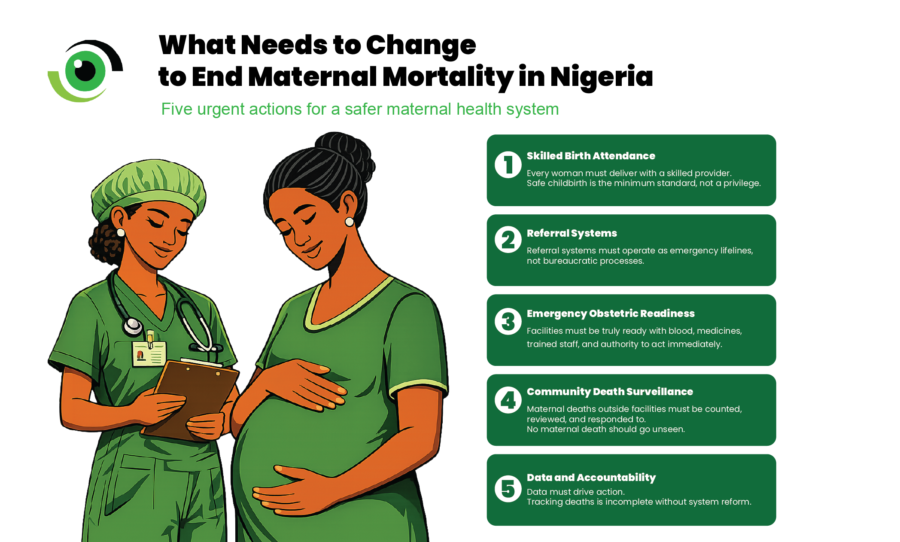
Referral systems must function as emergency networks, rather than administrative pathways. WHO guidance on Emergency Obstetric and Newborn Care emphasises the importance of timely referral, functional transport systems, and effective communication between levels of care. Reliable transport, designated referral centres, real-time coordination, and clear accountability for breakdowns are critical to preventing avoidable deaths.
Emergency obstetric readiness must reflect actual functionality. Facilities need skilled staff on duty, access to blood transfusion services, uterotonics, and magnesium sulfate, and the authority to act without delay. Persistent deaths from postpartum haemorrhage (PPH) and eclampsia point to failures in response, not diagnosis. Community maternal deaths must be fully integrated into surveillance and response systems. WHO’s MPDSR framework explicitly calls for the inclusion of community-based deaths that occur outside facilities to enable a complete and accurate understanding of the problem. Without this, responses will continue to address only part of the picture.
Finally, data must drive corrective action. Global strategies on maternal mortality make clear that surveillance systems are only effective when linked to accountability and system reform. Initiatives such as MAMII improve visibility, but visibility alone does not save lives. Impact depends on whether identified gaps lead to sustained changes in staffing, financing, referral readiness, and service delivery.
Maternal deaths in Nigeria are not inevitable. They persist where proven interventions are applied inconsistently. The true measure of reform is not policy design, but whether women survive childbirth.