
Zubaida Baba Ibrahim [Lead Writer]
Since the onset of the COVID-19 pandemic in 2020, immunisation efforts in Africa have experienced a significant setback, leading to a concerning increase in the number of unvaccinated and under-vaccinated children on the continent. Nigeria and Ethiopia have the highest numbers of unvaccinated children in Africa, with a combined total of over 3.3 million children who have not received any vaccines.
In this insightful interview, Dr Ephrem T. Lemango, Associate Director of Immunisation at United Nations Children’s Fund (UNICEF), sheds light on the persistent challenges facing routine immunisation and vaccine coverage in Africa. He also offers valuable strategies for countries and communities across the continent to overcome these hurdles and improve vaccination rates.
Can you explain the current state of childhood vaccinations in Africa and why the continent has the highest number of unvaccinated and under-vaccinated children?
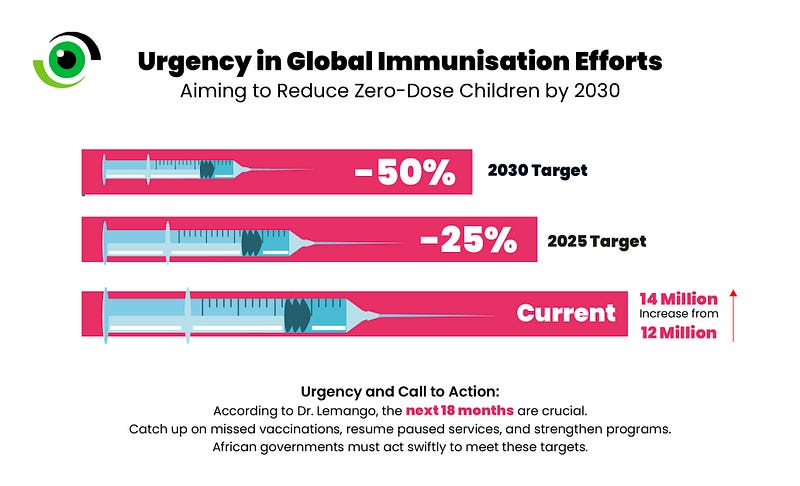
Dr Lemango: “Due to the COVID-19 pandemic, health workers had been diverted to respond so there has been a decline in the attention given to immunisation and the resources of immunisation [worldwide]. As a result, in 2021 the overall coverage of immunisation declined significantly. The past two years we have seen some recovery albeit driven by [relatively] larger countries like India, Indonesia, Brazil and a few large African countries like Tanzania these improvements have pushed the overall number of zero-dose children to decrease significantly so we moved from about 18 million unvaccinated children in 2021 to 14 million in 2022. Unfortunately, there is a key challenge: the change in zero-dose children is stagnant in Africa despite improvements in other regions.

Secondly, children that were missed [during] the years of the pandemic starting from 2019 which would have been caught-up in 2020 –but couldn’t be caught up because the pandemic–required concerted effort to catch them up. This has resulted in about 80 million under-vaccinated children [globally], out of which 60 million are zero-dose.
It is also prominent in Africa due to conflict and fragility. Children who live in areas and settings where there is a significant number of conflicts tend to miss out on immunisations because service delivery is usually affected due to people getting displaced. Also, service delivery is not safe for health workers, so they are not there. Research shows that [at least] 40% of zero-dose children in Africa live in conflict affected areas.”
What role does misinformation or vaccine hesitancy play in the under-vaccination of children in Africa and how can it be tackled?
Dr Lemango: “The best way to look at vaccine-confidence, is like a spectrum, in the sense that on one end there is an entire anti-vax movement –which outright rejects vaccines– and on the other end there are people who accept vaccines regardless. And then you have all sorts of people in between who just require clarity, to understand the use of vaccines, and whenever they have questions, the ability and the readiness of the system to respond to those questions. People will become hesitant when they don’t have enough information on the impacts and side effects of the vaccine. This requires engagement with the health workers, someone explaining to them the importance. But if they are not willing to take the vaccines due to influence of, let’s say, a religious leader, then it does require negotiation and discussion with religious leaders.
One important thing to keep in mind is an overall mistrust on vaccines is usually not a solitary issue. It is usually born out of mistrust in the system, or mistrust to governments that govern the vaccines etcetera. One good example is the COVID-19 vaccines, where people who thought these vaccines came from the west to do XYZ things in other settings will be very uncomfortable, if you ask them to take COVID-19 vaccinations. So as much as there are investments needed to avail vaccines closer to communities and to bring vaccines to health facilities. It is equally important to invest in making sure communities understand the importance of vaccines.”
If there is a lack of confidence in where and how the vaccines are provided, would Africa’s ambition for self-sufficiency in vaccine manufacturing boost vaccine confidence and uptake on the continent?
Dr Lemango: “Africa’s vaccine manufacturing is an important aspect of making the continent self-reliant on the supply it needs to fulfil the demands of its people, so it is important to do that.
I think there is an estimate that by 2100, 4 billion people will live in Africa, while the rest of the world will continue to decrease in its population, and this will be met by the capability to be able to meet the needs of the continent. So, there are current efforts built to produce vaccines in Africa and this was born out of the challenges faced during the pandemic though many governments have been prioritising vaccine manufacturing even before COVID-19 and initiating a process to have private sector investments to produce additional vaccines.

So, it can play a role once it materialises and it can contribute to better confidence when people think the vaccine is being produced in the continent, but it [can] come with a question where some parents may ask how safe these vaccines are when they are produced in Africa.
It is [currently] hard to conclude because we have seen people that will say they prefer something produced in Europe or North America versus something that is produced in Africa. But if it is much closer [to people] and we can show that these are also manufactured in something that meets the standard, people could be trusted more.”
Can you discuss the strategies some countries are implementing, that Nigeria can learn from
to reduce the number of zero-dose children?
Dr Lemango: “Reaching zero-dose children starts with identifying where they are and this varies from context to context, and countries have employed several innovations including using Geographic Information Systems (GIS) to map out population clusters in remote rural areas. There have been so many ways to identify children, but the usual challenge is once they have been identified, how do we reach them?
This varies from place to place. For example, in Ethiopia, they have mobile health and nutrition teams –given that many children that miss vaccines are likely to miss other essential health and nutrition services. So, they organise these teams to be able to deliver these services on a regular basis and this has been adopted in many countries. There [are also] some working with private sectors in urban areas; private health service providers or private immunisation facilities to address some of the barriers in access to services in urban poor communities.
In Nairobi, Kenya, they have been able to organise outreach services for those in urban informal settlements, whereby a group of health workers work with these settlements on a regular predictable schedule. In conflict areas we have seen negotiating access whereby organisations like International Committee of the Red Cross (ICRC), UNICEF and other partners do negotiations with non-state actors.”
What urgent actions can community-based groups and community members do to improve vaccine coverage?
Dr Lemango: “Community-based groups are like the glue that brings the government and communities together. So, they play a big role in creating trust on vaccinations and service delivery, they have that influence between community members for them to seek services and they can help to address concerns and confusions. And these groups have the potential to address [health] needs beyond vaccinations.
In countries where the governments are not able to avail services, community-based organisations play quite a strong role in working with communities and building resilience and respond to outbreaks.
Community-based groups can also hold governments accountable, by asking for health workers to be there, vaccines to be supplied, and escalating any issues to be addressed from the community level to the national and higher level. So, there is an advocacy role they can play, and it has been quite impactful especially those organisations that have a good public base can influence. So, community-based organisations can use advocacy to improve service delivery and create more trust within communities.”
Dr Lemango assumed his role at UNICEF Headquarters in June 2021, leading the organisation’s immunisation and vaccine-related efforts across seven regions and over 130 countries. With more than 15 years of experience in immunisation, maternal and child health, primary healthcare, and socio-economic development, Dr Lemango brings a wealth of knowledge to global immunisation efforts.
1 Comment