
Few global health and development interventions have yielded as profound an impact as vaccines. For over two centuries, these remarkable interventions have stood as a defence against vaccine preventable diseases such as polio, measles, and smallpox, enabling children to embrace a healthier, happier future filled with limitless possibilities. However, despite the long-established advantages, low rates of immunisation persist.
About 12 million children in low-income countries continue to be deprived of essential vaccines such as diphtheria, tetanus, and pertussis-containing vaccine. These zero-dose children account for almost half of all vaccine-preventable deaths globally.
Strengthening routine immunisation in northern Nigeria
In northern Nigeria, the distribution and uptake of routine immunisation (RI) had been hampered by several challenges, including poor cold chain and logistic systems, ineffective supportive supervision, unreliable data quality, insufficient community mobilisation efforts, weak human resource systems, and poor funding.
Recognising the urgent need to address RI performance in the region, between 2012 and 2016, six states — Bauchi, Borno, Kaduna, Kano, Sokoto, and Yobe States — signed Memorandums of Understanding (MoUs) with the Aliko Dangote Foundation and the Bill & Melinda Gates Foundation, to drive political and financial commitments and accountability in RI and primary health care (PHC). Through the MoUs, state governments and partners contributed funds into dedicated state-managed programme accounts (basket funds) to finance RI over a 10-year period which ended in 2022.
According to Dr. Raihanah Ibrahim, Principal, Solina Centre for International Development and Research (SCIDaR), the aim of the ‘Northern Nigeria States Routine Immunisation Strengthening’ project (NNRISP), which is SCIDaR’s flagship project, was to support the six states in strengthening RI structures and improving the immunisation outcomes in these states. “The implementation of the MoU has enabled us to provide ongoing technical support to the states in effectively managing the MoUs and routine immunisation programmes while also focusing on capacity building for state-based teams,” she added.

The support provided by SCIDaR encompassed technical support for the implementation of the MoU across seven thematic areas:
- Governance & Coordination
- Community Engagement
- Monitoring & Supportive Supervision
- Capacity Building
- Vaccine Supply Chain & Logistics
- Accessibility & Utilisation
- Financial Management

Platforms like the State Taskforce on Immunisation (STFI), which has now evolved into the State Taskforce on Primary Healthcare, were established and supported to provide comprehensive oversight for coordination and instituted bi-annual high level programme reviews with the MoU principals.
What’s Working
CRoWN Initiative: Enhancing Immunization Uptake for Zero-Dose Children in Bauchi State
The Community Reorientation Women Network (CRoWN) initiative is working to increase immunization rates among children by leveraging trained community volunteers to identify zero-dose children and help connect them and their families with vaccination resources. Three months into the initiative’s pilot phase, CRoWN volunteers managed to reach 99% of identified zero-dose children, leading to increased vaccination rates among youth.Read more
Incorporated into the governance structure were coordination frameworks like the State Emergency Maternal and Child Health Intervention Center (SEMMCHIC) and the State Emergency Routine Immunisation Coordinating Committee (SERICC). In addition, a range of specialised technical working groups were established — service delivery, monitoring and evaluation, finance, vaccine supply chain, community engagement, and training. In collaboration with partners, these groups worked together to develop eight fully costed annual workplans in each state to mobilise tools and resources for the implementation of routine immunisation and primary healthcare.
Furthermore, in line with the National Reaching every Ward (REW) strategy, which aims to provide regular, effective, quality, and sustainable routine immunisation services in every ward, the project supported the creation, implementation, and integration of micro plans at the ward level and these were subjected to quarterly desk reviews.
SCIDaR played a pivotal role in the success of the NNRISP by facilitating a data-driven expansion of vaccination services to delivery sites across both public and private healthcare facilities in the supported states. They also worked closely with the states to develop and implement special interventions targeted at reaching underserved communities. One notable example is the CRoWN Initiative.
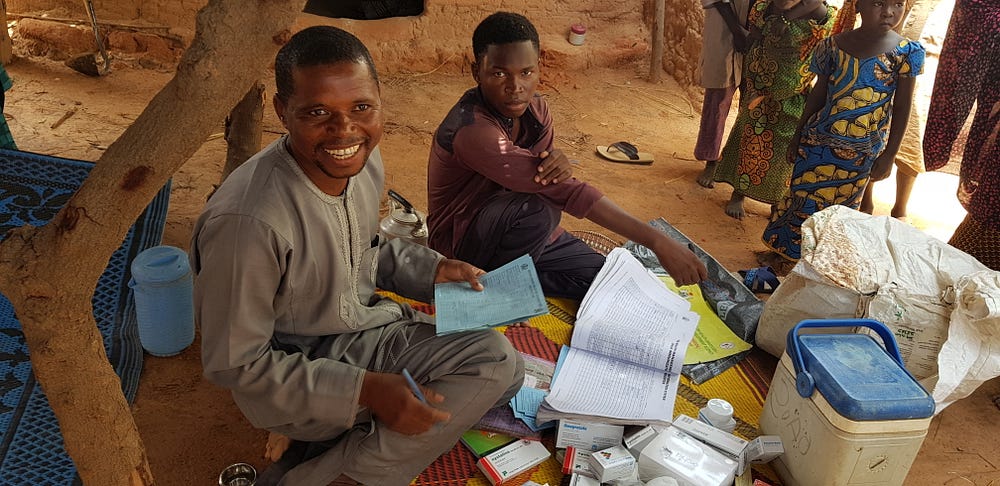
Photo Credit: Solina Centre for International Development and Research (SCIDaR)
States were provided with technical assistance for the effective use of government and donor funds. State Primary Health Care Development Agencies (SPHCDAs) received technical support on budgeting, disbursement, expenditure tracking, and reporting. The project through the implementing partners also facilitated transition to electronic payment systems to ensure direct payment to the last mile. Financial retirement tools to report expenses were developed, and state finance working groups were established to coordinate financial management systems.
To improve data integrity and its effective utilisation, SCIDaR, in collaboration with McKing Consulting Corporation, African Field Epidemiology Network (AFENET), the World Health Organisation, and other partners, designed and implemented monthly local government area (LGA) data validation and review meetings, which served as a platform for validating and ensuring the accuracy of collected data. Monthly state-level programme review meetings were introduced to facilitate data-driven decision-making at a higher level. Quarterly data quality assessments were initiated to assess and address any gaps or inconsistencies in data quality. The reporting system was also transitioned from the District Vaccine Data Management Tool (DVDMT) to the National District Health Information System (DHIS2), ensuring standardised and streamlined data reporting.

Photo Credit: Solina Centre for International Development and Research (SCIDaR)
To strengthen data control and management, a data control room was established, providing a centralised hub for monitoring and improving data quality across various levels of the healthcare system. These interventions collectively aimed to enhance the reliability, accuracy, and utility of data for informed decision-making and programmatic action.
Building capacity and engaging communities: empowering health systems for immunisation
Bauchi State signed the MoU in 2014 and has since worked towards strengthening the state’s RI structures. Dr. Rilwan Mohammed, Executive Secretary, Bauchi State Primary Health Care Development Agency said, “Working closely with the State Primary Health Care Development Agencies (SPHCDAs), we have strengthened existing structures and systems and established new ones as necessary”.
According to Dr. Musa Usman Matazu, a McKing consultant supporting the project implementation in Yobe State, “Five years into the implementation of the MoU, the indices have improved, and we have seen the increase in Immunisation coverage from 9 percent in 2013 to 51 percent in 2018.”
As a sustainability measure, capacity building of state-based staff was made a priority, and the project successfully built the technical capacity of about 102 State Primary Health Care Development Agencies (SPHCDAs) and Ministry of Health staff across the MoU States.
Additionally, over 422,195 traditional leaders participated across all the states, raising awareness and promoting the importance of immunisation within their communities.

Navigating obstacles and sustaining gains: lessons learned
However, several challenges were encountered during the project’s implementation, which impacted its overall effectiveness and outcomes. Sub-optimal supervision and weak oversight at the LGA contributed to a breakdown in the translation of programme objectives, leading to weaknesses in service delivery. Socio-cultural factors such as poverty, illiteracy, and prevalent myths also posed challenges to the acceptance and uptake of immunisation within communities.
Nevertheless, the project greatly benefited from the unwavering political will of the governments of the six northern states supported by SCIDAR, who displayed a strong commitment to enhancing RI coverage. This commitment was evident through the allocation of substantial financial resources, the establishment of robust RI systems, and the active involvement of community leaders.
NNRISP serves as a testament to the transformative potential of collaborative partnerships, technical expertise, and dedicated political will. Particularly, the implementation of a funding structure that assigned specific funding responsibilities to each signatory throughout the duration of the MoU. This framework facilitated a gradual transition of funding responsibility from the partners to the government, culminating in the government assuming 100% of the funding by the end of the MoU.
Dr. Ibrahim underscored the importance of capitalising on the insights gleaned from the execution of the Memorandums of Understanding (MoUs) and expanding their scope to include a broader range of primary healthcare services in the states. Through the application of these insights, the overarching functionality of primary healthcare systems can be elevated.