
Tzar Oluigbo (Lead writer)
On a dusty afternoon in Rafin Bauna, a community in Aleiro Local Government Area of Kebbi State, Rashida Abdullahi, a Volunteer Community Mobiliser (VCM), adjusts her veil and steps into another compound. She has already visited three homes today. In one, a mother asked what to do if a child develops a mild fever after vaccination. In another, the mother agreed but said her husband would decide whether their child should receive the vaccine. In many settlements, demand for routine immunisation is built less through campaigns and more through patient, repeated conversations at the doorstep that help families understand vaccination and make confident decisions for their children.
For Rashida, a mother of six, immunisation is personal. When her third child was born in 2020, her husband did not agree to vaccinate the baby. Her daughter later became seriously ill and needed hospital care. Rashida said that, in the same period, a neighbour’s vaccinated child did not fall ill, a contrast that stayed with her and strengthened her resolve to keep advocating at home. When community mobilisers later visited with a counselling flipbook explaining each vaccine and the schedule page by page, her husband agreed.
Three times a week, she visits households in the mornings or afternoons, reminding caregivers about sessions and encouraging them to bring children for vaccination. “If the mother agrees and the father refuses, I don’t argue,” she said. “I involve the community leader so we can discuss concerns calmly. Sometimes it takes more than one visit.” Across wards and settlements, women mobilisers go door to door, and traditional birth attendants (TBAs) help bridge a long-standing gap by identifying newborns after home deliveries and linking families to routine immunisation services.

From Isolation to Community Mobilisation
For years, routine immunisation in many communities depended on families coming to the primary health care (PHC) facility, and too often they did not return. The distance to the health facility, indirect costs such as transport fares, time away from work or trading, and trust shaped whether caregivers returned for follow-up doses. In many households, fathers or elders influenced children’s health decisions, and rumours about vaccines could spread faster than accurate information.
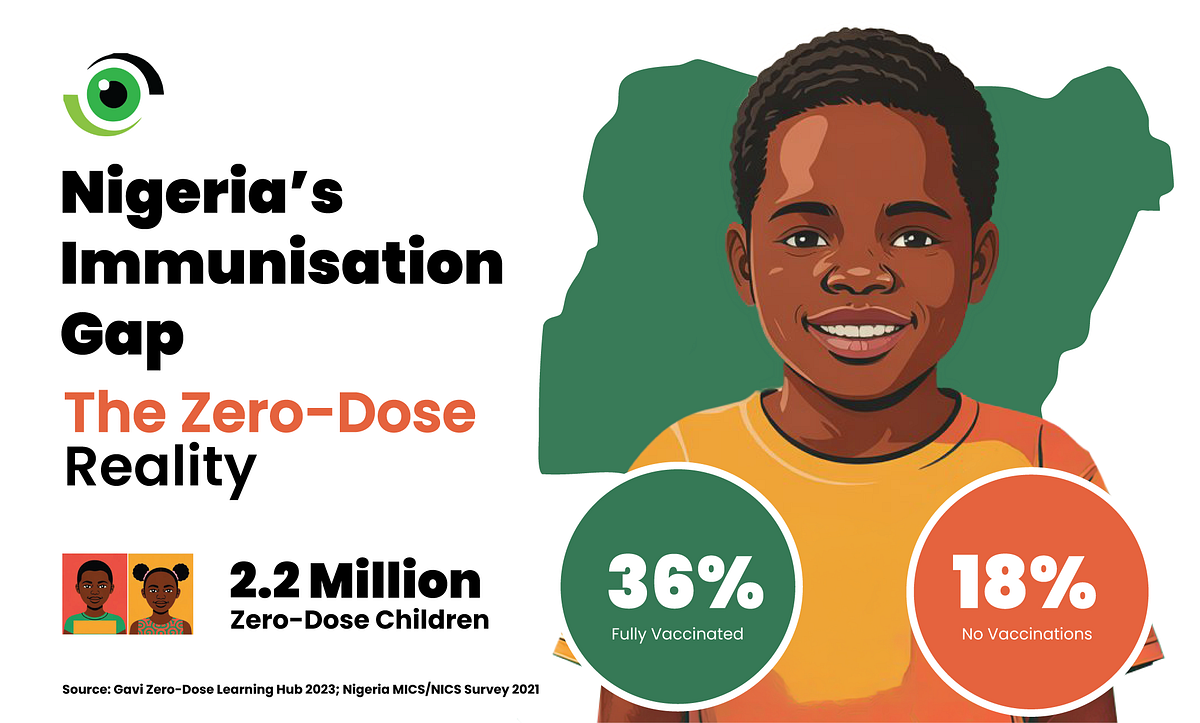
In Nigeria, only 36% of children 12–23 months receive all recommended vaccinations, 18% receive none, and an estimated 2.2 million children receive no vaccinations at all. In this context, VCMs were introduced. VCMs are selected from the communities they serve and trained to conduct house-to-house counselling, track newborns, follow up missed children, and link families to routine immunisation sessions. In Nigeria’s polio programme, similar community mobilisation contributed to fewer missed children and fewer household refusals, a lesson routine immunisation is now trying to institutionalise.
Alongside VCMs, Mama-to-Mama groups organise women at the settlement level for peer learning, reminders, and problem-solving around breastfeeding, hygiene, antenatal care, and immunisation. TBAs were not pushed aside. Instead, where home deliveries continue, TBAs can help notify the health facility about births so newborns are registered and followed up for vaccines. Kebbi State’s health sector plan flags severe child health burdens and positions community mobilisation as necessary to improve uptake of essential services. Immunisation should not be left to clinics, but must be built into a community system.
Progress and the Cost of Interrupted Support
Like many community-based interventions, long-term sustainability depends on stable financing and local ownership. “When the VCM work started, we shared the idea and communities accepted it,” said Alhaji Yusuf Umar Sawwa, the State Health Promotion and Education Officer. He said UNICEF later supported the programme with stipends. Mobilisers report receiving ₦20,000 per month. At the same time, Mama-to-Mama groups that were not given any stipends were strengthened through organised contribution schemes at ward and settlement levels.

Women contributed weekly or monthly and took turns collecting the pooled funds to start small businesses. The support did more than provide income; it gave the women confidence and a stronger voice in their communities. “In one community, a woman was able to rear cattle, selling one cow for ₦500,000 through the money she got from the contribution system to rear cows,” Sawwa said.
Gradually, change became visible as more mothers started attending antenatal clinics, immunisation reminders became more consistent, and community leaders stepped in when fathers resisted vaccination, showing that mothers were becoming more confident in making decisions about their children’s health. In some health facilities that were once nearly empty, women began showing up regularly for immunisation days. But these gains were not immune to funding challenges. Rashida explained her routine, “Since 2020, I have worked across three communities and followed up with many families,” Rashida said. “When stipends were paid, we could keep visiting. When payments stopped, many of us reduced visits because transport and time costs became too heavy.”
For women who are navigating economic hardship, volunteering without support is difficult to sustain. Many VCMs are mothers with households to manage, and with rising transport costs and the need to spend time away from petty trading or farming, the result is often lost income. Sawwa further explained that “The funding cut in January 2025 put an end to the stipends. These women are committed, but they also have families to support. When the stipends ended, some had to step back. It is difficult to sustain community mobilisation without consistent backing, so we are trying to introduce the contribution system to them too”.
In Kebbi, the story is no longer about the absence of effort; it is about whether the support behind that effort can keep up with the progress it has begun to generate. Kebbi’s PHCs are functional, but utilisation remains uneven. “Health facilities are there,” Sawwa said, “but people prefer to go to chemists.” To reach children in hard-to-reach settlements, the state provides ₦4,000 per facility per month to support a health worker for immunisation outreach, roughly ₦1,000 per week. The intervention has been running for five years, but inflation has eroded its value. One health worker lamented that ₦1,000 is not enough, noting that his monthly salary is ₦28,000 and that he spends ₦1,000 daily on fuel for his motorcycle just to reach the facility.
Working with Tradition, Not Against It
At Rafin Bauna PHC, Chief Nurse & Midwife Hafsatu Bawale Haliru has worked for years but has never conducted a delivery at the facility. “We try to work with TBAs,” she explained. “When they conduct home deliveries, they bring the names of mothers and newborns for registration and immunisation.” This relationship, once informal, is becoming strategic. TBAs now serve as referral links into the health system, especially for postnatal care and immunisation tracking. “Those traditions where a woman believes if she comes to the hospital, there will be complications…that is what is stopping them,” she further explained.
In Kebbi, this is becoming more than just an immunisation effort. It is taking shape as a layered approach that includes:
- VCMs conducting household counselling, newborn tracking, and reminders.
- Mama-to-Mama groups supporting peer learning and practical problem-solving.
- TBAs identifying newborns after home deliveries and linking families to PHCs.
- Community and religious leaders convening dialogue where resistance persists.
- Health workers delivering fixed and outreach sessions, despite operational constraints.
But for this to become a true routine immunisation strategy rather than a fragile project, three actions are urgent:
- Define the indicator and publish local results. Track and communicate progress using clear measures (zero-dose, Penta1–Penta3 dropout, and full basic immunisation). Nigeria’s zero-dose analysis shows why these definitions matter.
- Ring-fence predictable financing for community follow-up. Use BHCPF and state PHC budgets to fund supervision, transport, and the operational backbone of mobilisation, not as an occasional allowance, but as a routine function.
- Treat trust-building as a health system task. Equip mobilisers and health workers with standard messages on vaccine safety and side effects, and ensure caregivers who report concerns are respected and supported.
In Kebbi State, women like Rashida are already doing the hardest part, which is turning fear into conversation, and conversation into action. The question now is whether government systems will do their part by funding the routine work that keeps children protected long after the campaign banners are gone. Kebbi’s approach already demonstrates what is possible when immunisation is treated as a community system rather than a facility service.
By working through Volunteer Community Mobilisers, strengthening Mama-to-Mama networks, and engaging TBAs rather than sidelining them, the state is building a locally rooted model of demand generation, with the potential not only to improve routine immunisation coverage but also to strengthen maternal and child health outcomes more broadly.