
Shehu Muhammad Shehu (Lead writer)
For Sadiya Abdullahi, a 35-year-old mother of three in Zugu in the Bukkuyum Local Government Area of Zamfara State, getting care has become a dangerous journey. When her young son fell ill in November 2025, the community’s primary health care (PHC) facility was not providing services. Like many residents, she first went to a local chemist. When his condition did not improve, she travelled more than 30 kilometres to Gummi General Hospital, using bush routes she described as unsafe because of bandit attacks. “Even after injections, his stomach kept swelling, and they told me he was malnourished,” she said.
Zamfara is one of the northwestern states experiencing ongoing armed attacks and kidnapping for ransom. Community members in Zugu said that insecurity has decreased farming and trading, reducing income just as the cost of reaching healthcare rises. What is happening in Zugu is not only a security story; it is a primary health care delivery failure, where closed PHCs are turning routine care into dangerous travel, late referrals, and preventable maternal and newborn deaths. For pregnant women, the impact is particularly severe. Sadiya said many women now deliver at home with untrained attendants because nearby facilities are either closed or cannot provide basic maternity care. During pregnancy, when she visited the Zugu PHC, she could not receive antenatal care (ANC). “There was no blood pressure check, no weighing scale, nothing,” she said.
Surajo Marafa, the district head of Zugu, said that local health services have been declining for years, but they worsened dramatically after major attacks in 2023. He mentioned that some villages have been abandoned. “Places like Takalafiya are now empty. Others, like Kyaram, cannot even access a mobile network, let alone a health facility,” he said. He explained how residents transport emergency cases by motorcycle along bush paths to reach care in nearby towns such as Gadar Zaima, Daki Takwas, Maga, Gummi, or Bukkuyum. “Last week, a pregnant woman from Kairu died before reaching the hospital,” he said, adding that a functioning PHC could have improved her chances of survival.

An empty clinic in a high-risk community
Zakariya Muhammad, the officer in charge of the Zugu PHC, has worked there for more than 15 years and recalls when the facility was functioning well. “We had blood pressure machines, weighing scales, and basic laboratory equipment. We supported tuberculosis treatment, admitted patients from nearby villages, and handled some labour cases,” he said. He added that the PHC once served more than 50 surrounding villages. Today, the building is dilapidated, the ceiling is rotting, the doors are broken, the windows are shattered, and the wards have no beds. In the pharmacy, shelves are mostly empty, except for malaria test kits and artemisinin-based combination therapies (ACTs) donated by an NGO. He said many staff stopped reporting for duty after repeated attacks and threats. As residents fled or avoided travel, attendance dropped sharply. “Sometimes I spend the whole day without seeing a single patient,” Zakariya said.
For Sumayya Sa’idu, 27, who is pregnant with her fourth child, the absence of care turns common illness into an emergency. “Last week I had a fever. I went to the PHC, but nobody was there,” she said. “I travelled to Gummi and spent ₦6,000 on transport and more than ₦7,000 on medicines.” In Balhe village, residents said they cannot even reach Zugu because of the risk of attacks on the route. A community leader, Hakimi Yelmo, estimated that between 600 and 700 residents have no reliable access to any health facility. “We took a woman in labour, but she delivered on the road before we reached Zugu, and the baby did not survive,” he said. The disruption also affects routine immunisation. Balhe has no vaccination point, meaning parents must travel to Zugu for routine immunisation despite the PHC’s limited services. Even when families can afford the fare, insecurity along the route can delay or prevent clinic visits, increasing the risk of missed vaccinations.
Why clinics close when communities become unsafe
Experts say insecurity is a major driver of Zamfara’s health crisis. Dr Tijjani Shinkafi, a senior lecturer at the One Health Institute, Usman Danfodiyo University, Sokoto, said armed violence has severely weakened rural healthcare across parts of northern Nigeria. “When communities become unsafe, health workers, especially non-local staff, may be unwilling to stay. This creates chronic shortages, leaving facilities unstaffed or barely functional,” he said. He added that insecurity can also disrupt supply chains, preventing essential medicines from reaching rural facilities. With insecurity disrupting rural health services, Nigeria and affected states such as Zamfara need a practical protection plan for healthcare in conflict settings, aligned with the World Health Organization guidance on protecting healthcare in armed conflict.
The state government, through the Zamfara State Primary Health Care Development Agency, needs to maintain a conflict-adapted minimum service package for PHCs, including ANC basics, routine immunisation, malaria case management, and a functioning referral pathway. In practice, protecting healthcare must mean providing services that people can actually access. Zamfara State and federal authorities should adopt a conflict-sensitive minimum service package for PHCs such as antenatal care, routine immunisation through fixed and outreach sessions, reliable malaria diagnosis and treatment, and a referral system that operates around the clock.
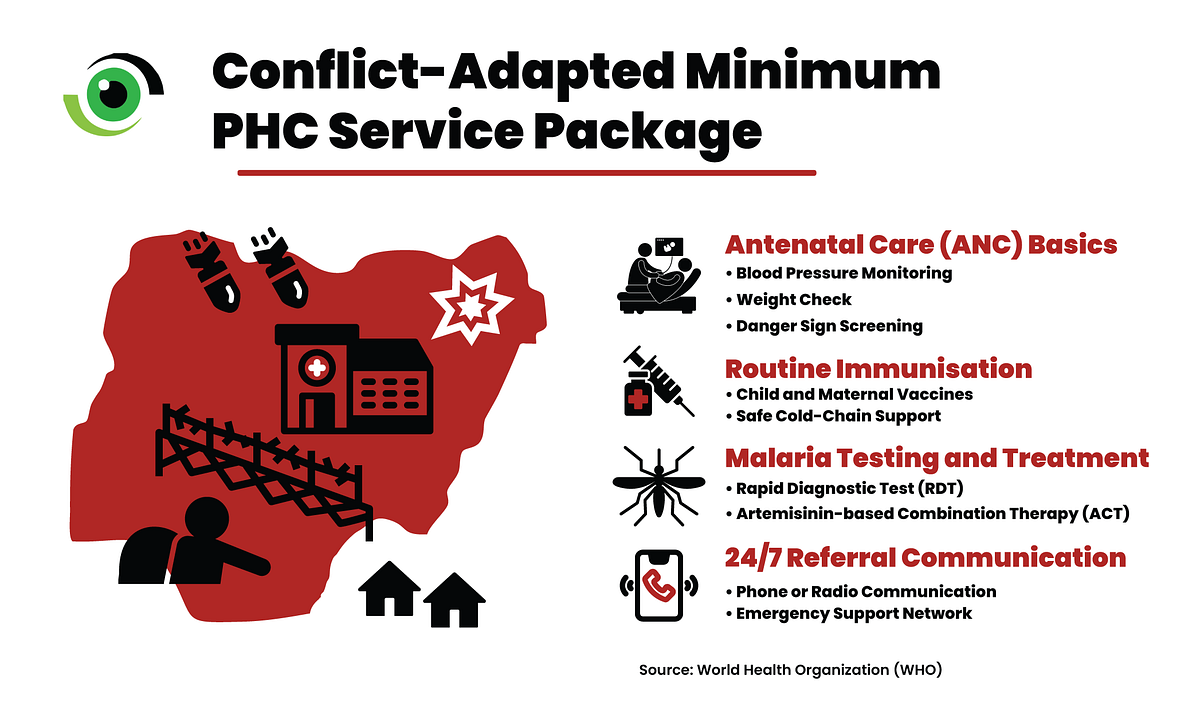
This requires practical actions such as risk mapping, planning safe routes with communities, staffing models that prioritize local recruitment and hardship support, protected drug and vaccine deliveries, and an emergency transport system that is funded and accountable. If PHCs cannot operate in insecure areas, mothers and babies will continue to suffer from a crisis they did not cause. A state cannot claim progress toward universal health coverage while entire communities risk traveling on dangerous bush roads to access care.