


Solomon Yemi Oladimeji (Lead writer)
In Northern Nigeria, where health systems often come face to face with socio-cultural beliefs, change does not arrive in white coats or government-issued badges. It comes in sandals, sits on prayer mats, and speaks the local language.
April 2025 was not just another month in Nigeria’s long battle against polio; it marked a renewed push to ramp up efforts. This time, it was not just about vaccines. It was about listening; about showing up again and again, in compounds, town halls, mosques, and marketplaces. It was about relationships, it was about trust and it worked.
Although Nigeria was declared free of the wild poliovirus in 2020, the continued emergence of circulating vaccine-derived poliovirus type 2 (cVDPV2) means the battle is far from over. Across eight northern states, Sokoto, Kano, Katsina, Kebbi, Zamfara, Jigawa, Yobe, and Bauchi, the situation remains especially critical. These states account for most of the nation’s polio vaccination non-compliance, driven by deep-seated distrust, misinformation, and limitations on the health system.
The cVDPV2 strain is a mutated form of the weakened poliovirus used in the oral polio vaccine. In communities with low immunisation coverage, the weakened virus can continue to circulate from person to person, eventually mutating into a strain that behaves like wild poliovirus, capable of causing paralysis. It spreads through contaminated water, poor sanitation, and contact with faeces.
As part of the National Immunisation Plus Days (NIPDs), Nigeria Health Watch, in collaboration with the National Primary Health Care Development Agency (NPHCDA), Solina Centre for International Research and Development (SCIDaR) and other partners, deployed civil society organisations (CSOs) across high-risk states.


While the immunisation campaign took place across several states, Bauchi and Kebbi were where Nigeria Health Watch focused its efforts. In these states, April 2025 marked a significant shift. This round of the National Immunisation Plus Days (NIPDs) was not just another campaign, it was a recalibrated response to persistent gaps that threatened to reverse hard-won gains. It was the moment Nigeria resolved to listen louder than it spoke. The real strength lay not in the deployment, but in the way it was designed. A strategy built on one key element, stakeholder buy-in.
Royal endorsements and religious allies
The campaign in Kebbi State opened with the Emir of Argungu publicly vaccinating his children, a rare and powerful gesture in a region where leadership is more than symbolic, and carries deep influence. In Bauchi, a similar scene played out. Religious clerics were engaged early and trained not only on vaccine facts, but on how to address theological concerns in Friday sermons. When an Imam stands before his congregation and speaks of vaccines as Amanah — a trust from God, it reframes immunisation not as foreign imposition, but as divine responsibility.


This model challenges recent global criticism. Reflecting on Nigeria’s public health performance, Bill Gates, Chair of the Gates Foundation observed that the country’s health outcomes could be significantly better, especially in the northern states, which lag behind Sahel countries such as Mali, Burkina Faso, and Niger in vaccination coverage. He noted that, “more children live in northern Nigeria than in all those other countries combined, and that’s where we have the lowest vaccination rates in Africa. Even lower than Somalia.
Compound by compound: Where the real conversations happen
In Kardi Ward, Birnin Kebbi, the capital city of Kebbi State, CSOs arrived at a family compound where the gate had remained shut through three previous campaigns. However, this time, we were not strangers. A CSO mobiliser who had grown up in the same ward came along, and instead of arguing, we listened.
Under the shade of a neem tree, over cups of Shayin Buzaye — a traditional spicy tea, we spoke of children, of fear, of faith. Eventually, the fathers leaned back, pointed to their sons, and said simply, “Ku yi musu,” — give it to them.


Image credit: Nigeria Health Watch.
These conversations were not accidental, they were planned, patient, and deeply personal. Microplans developed by CSOs included lists of compound heads, influential elders, and previously missed households. Every visit was logged, and every hesitation became an opportunity for more dialogues not debate.


Image credit: Nigeria Health Watch.
A combination of town announcements, edutainment, comic teams and visibility
Traditional communication also played its part.In Gwandu Local Government Area (LGA) of Kebbi State and other prioritised LGAs such as Jega, Koko/Besse, Yauri, Suru, Wasagu/Danko and Sakaba, as well as in Bauchi State across Kirifi, Darazo, Giade, Katagum, Ningi and Toro, CSOs partnered with drummers and town criers to ensure the campaign was not only known but celebrated.


Market days became platforms for education, with comic teams popularly known as Papalolos accompanied vaccination teams, turning routine health outreach into community spectacle.
Radio jingles aired three times daily in Hausa and Fulfulde, while town announcers made rounds with megaphones, reinforcing messages of safety, protection, and community pride. These were not mere media outputs, they were cultural interventions.
Real-time data, real-time action
Using Open Data Kit (ODK) tools, CSOs recorded every activity, from advocacy visits to resolving compound-level issues. When a case of noncompliance emerged, it triggered an immediate alert. In Kebbi, we noticed that one ward had shown a sudden rise in resistance. Within 48 hours, a joint team of CSO mobilisers, Non-Compliance Resolution Teams (NCRTs), and a community leader visited the hotspot. By the end of the week, 86% of the previously missed children had been vaccinated.
This approach was not just reactive, but also responsive with feedback loops built into every phase to ensure the system adapted in real time.


Image credit: Nigeria Health Watch
The numbers tell a story — but trust tells it better
Across the eight targeted northern states, 285,856 cases of noncompliance cases had been recorded in previous rounds of polio campaigns. In the April 2025 round alone, over 76% of these cases were resolved, with Kebbi leading at 92%, followed by Sokoto at 91%.

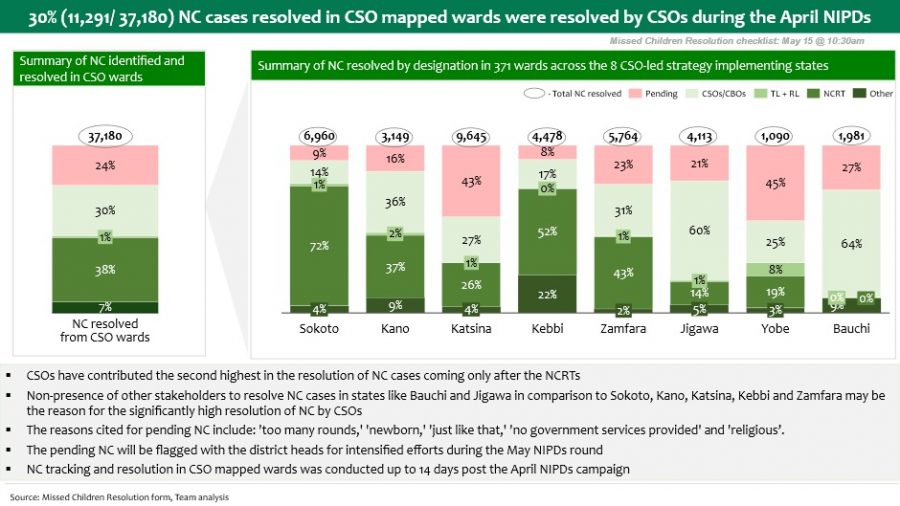
During the April NIPDs In Kebbi, over 69% of resolved noncompliance cases were handled by CSOs, traditional leaders, and religious leaders. In Bauchi, CSOs still led the charge, resolving over 64% of documented cases. Each number represented children protected, families reached, narratives reshaped and communities brought closer to eradication.
In one courtyard in Jega LGA, Kebbi, a father who had dismissed vaccinators for years finally called us over. What changed? It was not the message. It was the messenger. A CSO mobiliser he trusted, an Emir he admired, an elder he respected.
The campaign’s success lay not in shouting louder, but in listening better.
What’s next?
As preparations begin for subsequent immunisation rounds, the lesson is clear: stakeholder buy-in is not optional, it is fundamental. Compound meetings are not supplementary, they must be central in last-mile delivery of immunisation programmes . Community dialogues and town announcements are not “nice-to-haves”, they are the infrastructure of trust that drives demand and ensures equitable coverage.
In northern Nigeria, where suspicion runs deep and access remains difficult, the most effective vaccine delivery strategy may be this: sit down, listen deeply, speak their language, and walk alongside them. In the fight against polio, trust is not a peripheral tactic, it is the decisive factor in eradication.