


Oladimeji Solomon Yemi (Lead writer)
Malaria in pregnancy remains one of the leading preventable causes of maternal anaemia, low birth weight, preterm delivery, stillbirth, and neonatal death. A baby born with low birth weight faces a higher risk of dying during the first year of life, and a mother with severe malarial anaemia faces a greater risk of death during delivery.
As the world observes 2026 World Malaria Day under the theme “Driven to End Malaria: Now We Can. Now We Must,” it comes at a critical moment for Nigeria. The tools and policy frameworks to protect pregnant women from malaria are already in place; what remains is consistent delivery.
Nigeria employs various strategies to prevent malaria during pregnancy. Preventive treatment is integrated into antenatal care (ANC) protocols; insecticide-treated nets are widely distributed; and public health messaging on malaria prevention has been widespread. On the surface, the framework is in place, but prevention is not built on availability alone; it depends on continuity, timing, and consistency.
It also depends on whether the health system can sustain itself across multiple points of contact, each with its own vulnerabilities. However, the impact of malaria in pregnancy does not wait for the health system to update its approach.
In sub-Saharan Africa, an estimated 12.7 million pregnant women are exposed to malaria infection each year, and the burden falls disproportionately on countries where coverage of preventive interventions is incomplete. Nigeria accounts for the largest share of that burden on the continent.
Continuity has been a long-standing issue
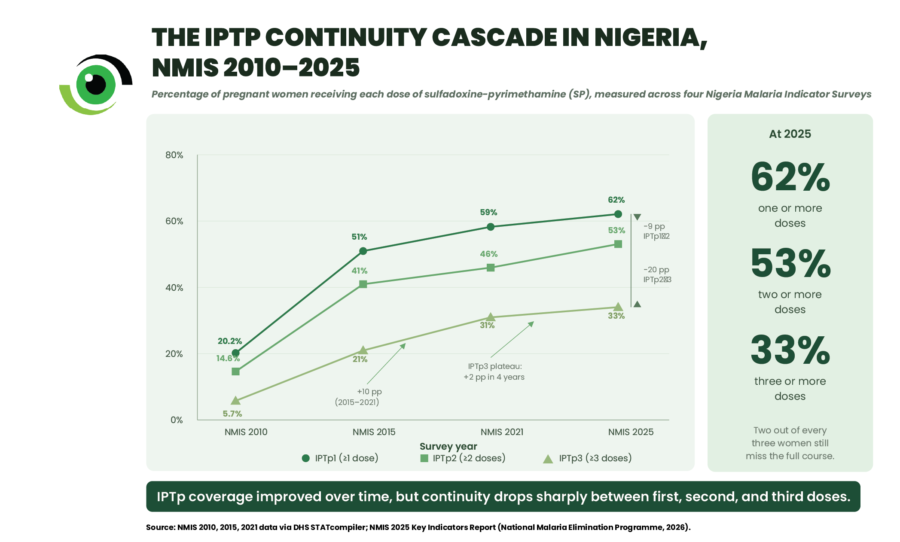
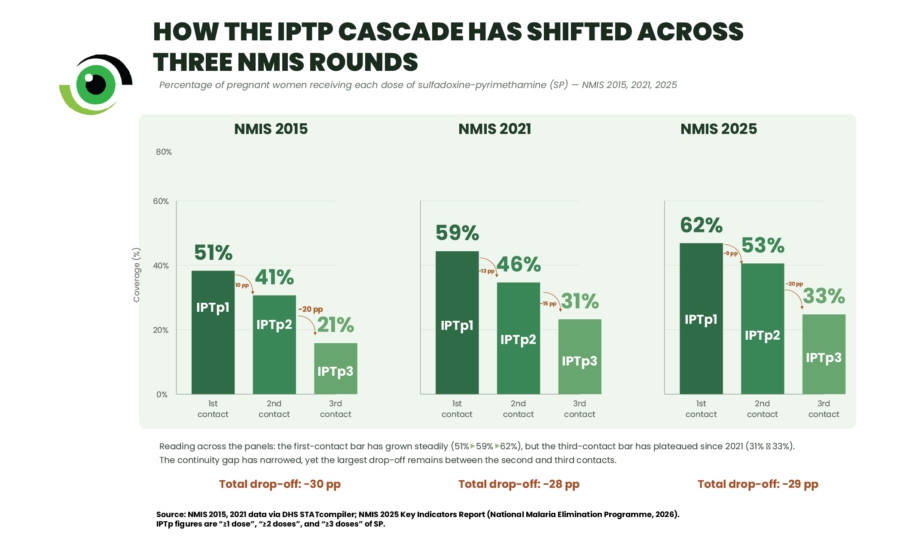
Available data consistently emphasise where the continuity of malaria interventions breaks down. In 2015, 51% of pregnant women in Nigeria received at least one dose of intermittent preventive treatment with sulfadoxine-pyrimethamine (IPTp‑SP); however, only 41% received a second dose, and just 21% received three or more doses, which the World Health Organization recommends for effective protection. Between the first and third contacts, coverage declined by 30 percentage points, revealing a gap in continuity that cannot be ignored.
By 2021, the third-dose figure had risen to 31%, marking the most significant single improvement in over a decade of survey data, and indicating that community-based delivery and strengthened coordination through the national Malaria in Pregnancy Technical Working Group are beginning to make an impact.
More recent data suggest that progress has continued, with coverage reaching approximately 33% by 2025, but this still means that two out of every three pregnant women in Nigeria do not complete the course that protects them.
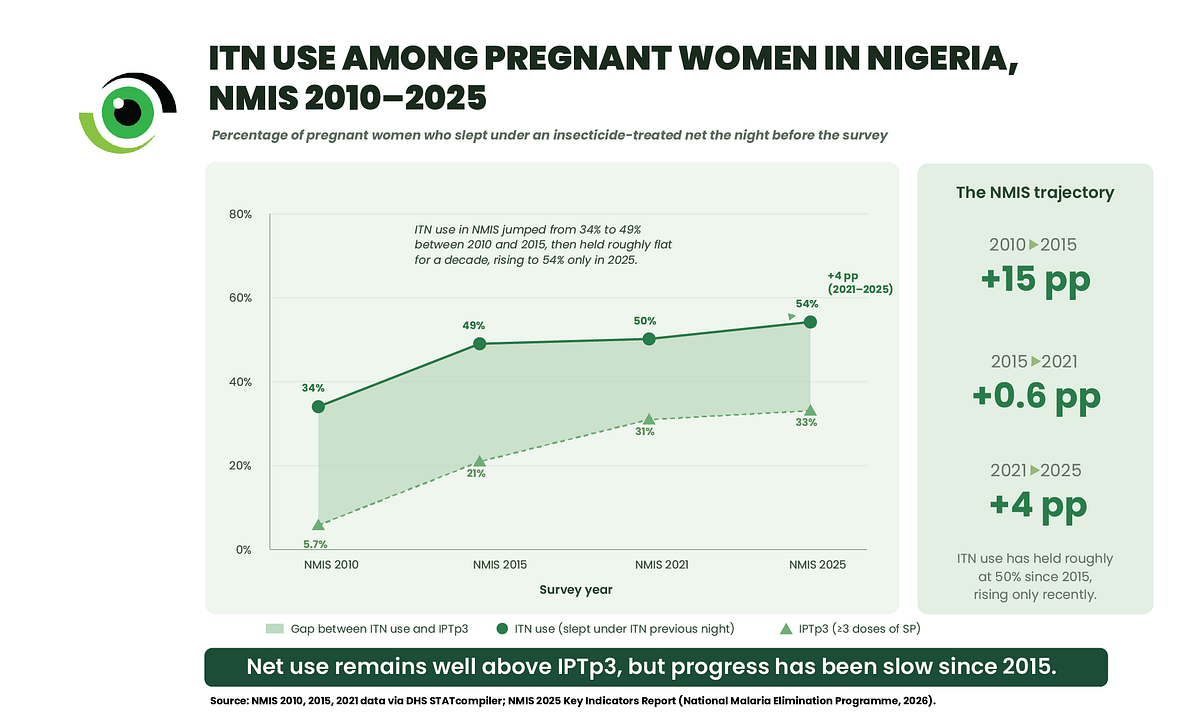
This pattern is not limited to preventive treatment. The use of insecticide-treated nets (ITNs) among pregnant women increased from 34% in 2010 to 49% in 2015 during the peak of the mass campaign era, but has since shown only modest gains, reaching 50% in 2021 and 54% by 2025. The initial acceleration has not been sustained, suggesting that while access improved during campaign periods, continuity of consistent use remains a challenge.

This decline results from a series of small yet cumulative breakdowns, such as many pregnant women receiving ANC late, often well into their second trimesters; facilities experiencing intermittent stockouts of sulfadoxine-pyrimethamine; and preventive treatment, even when prescribed, not always being given under direct observation.
Furthermore, follow-up visits are often missed or delayed, usually due to cost, distance, competing priorities, and previous experiences with the healthcare system. Although each of these issues may seem minor on its own, together they form a system that initiates protection but fails to sustain it.
The unevenness becomes more visible when analysed across states. Recent data from the 2024 Nigeria Demographic and Health Survey showed that ANC completion, the gateway to every subsequent malaria prevention step, varies by more than six times across the country.
In Lagos, 95% of women attend at least four ANC visits; in Osun, 92%; and in Anambra, 85%. These are areas where most pregnant women are reached early, and where the first dose of preventive treatment can usually be administered on time. However, even in these states, all located in the southern part of Nigeria, completing the full Intermittent Preventive Treatment in pregnancy (IPTp) course is not always assured.
The gap between starting and completing protection remains wider in the northern region. For example, in Kebbi State, only 14% of women complete four ANC visits. In Zamfara State, only 22%, and in Sokoto State, only 23%. Here, the challenge begins before protection can be provided at all, as fewer women are reached in time, and many never receive even the first dose. The issue can also be related to entry into care itself.
Between these two extremes, a third pattern exists. In some states, women start their ANC journey but do not finish it. The drop-off between the first dose of intermittent preventive treatment (IPTp1) and the third dose needed for effective protection (IPTp3) is steepest where retention is weakest, and retention is weakest where distance, cost, and confidence in the facility are hardest to overcome.
In practical terms, many women start preventive treatment but do not remain in care long enough to complete the doses that would fully protect them.

A similar contrast is seen in the use of mosquito nets. In some northern states, net use among pregnant women is relatively high, reflecting both availability and established use habits. In other southern states, nets are present in households but are used inconsistently.
The reasons are rarely captured in routine data, but qualitative studies across Nigeria and neighbouring countries have documented causes including discomfort from heat under the net, household sleeping arrangements that complicate consistent use, and the perception that risk is lower outside the rainy season.
Why strengthening continuity matters for what Nigeria does next
Strengthening continuity matters because it reframes what counts as success. A national coverage figure averages three very different system failures, each of which calls for a different response.
– Where the first contact does not occur (such as in Kebbi, Sokoto, and Zamfara), where fewer than a quarter of pregnant women complete four antenatal visits, the focus is on improving access, bringing services closer through community outreach, reducing travel and opportunity costs, and working through trusted local channels.
– Where women begin antenatal care but do not return (visible in parts of the north-east), the response is about completion, such as preventing stockouts of sulfadoxine-pyrimethamine, deploying community IPTp (cIPTp) alongside facility-based delivery, and following up missed appointments before they become missed doses.
– Where coverage is high but consistent use at home is lacking (such as in Lagos, Anambra, and Osun States), the response focuses on sustained behaviour: counselling that addresses the underlying reasons why women stop using nets, and more vigorous demand-side communication during every antenatal contact.
What this means in practice is that a uniform national approach will continue to leave the largest gaps untouched. The next phase of malaria-in-pregnancy programmes needs to be clearly differentiated, designed around which of these three patterns dominates in each state, and funded accordingly. That shift from uniform coverage to pattern-specific delivery is what truly requires serious commitment.
Now We Can. Now We Must
For pregnant women in Nigeria, this World Malaria Day, the theme “Driven to End Malaria: Now We Can. Now We Must” holds significant importance.
Now we can, because the tools and evidence already exist. Sulfadoxine-pyrimethamine works. Insecticide-treated nets work. Community-level IPTp delivery works, and the data show it.
Now we must, because the window for intervention is closing before the next transmission peak. Despite achieving 31% third-dose coverage in 2021 and approximately 33% in 2025, two out of three pregnant women in Nigeria still enter each malaria transmission peak without receiving the full course of protection they are entitled to.
The importance of continuity is not just theoretical. For the pregnant woman preparing for her first antenatal visit next month, and whose third visit will determine whether she completes the full course of care, the system must operate consistently. That is the true challenge for Nigeria on this World Malaria Day, and in the days that follow.