
Olaoluwa Olatunde (Lead Writer)
During my National Youth Service Corps (NYSC) in 2021, while I was posted to the National Health Insurance Scheme (NHIS) office a prominent government hospital in Abuja, an elderly woman, old enough to be my grandmother, approached me. She held in her hands a diagnosis form from her doctor, she urgently needed orthopaedic surgery.
Moved by the urgency of her condition, I immediately began the process of securing an approval code from the NHIS. Seconds turned into minutes, and minutes turned into hours, the patient remained seated in visible discomfort, waiting hopefully for a response.
Her procedure was eventually approved two days later. By then, her condition had worsened significantly due to the delay. This experience was not isolated. Over time, I encountered many similar cases where patients expressed frustration that accessing care through health insurance was often slower and more difficult than simply paying out of pocket.
Despite the promise of financial protection, many Nigerians with health insurance find themselves caught in bureaucratic delays that compromise quality and timely care. My experience, though deeply personal, reflects a systemic problem that has plagued Nigeria’s health insurance journey, since its inception. These bureaucratic delays undermine the core goal of Universal Health Coverage (UHC), which is to ensure equitable access to quality health services without financial hardship.
The journey to universal health coverage
The idea of establishing a National Health Insurance Scheme in Nigeria was first introduced in 1962 through a bill presented to Parliament by the then Federal Minister of Health, Dr. M. A. Majekodunmi. The concept was then revisited in 1988 by then Minister of Health, Professor Olikoye Ransome-Kuti with renewed effort that led to the development of the Eronini Report in 1989, which served as the foundational framework for the NHIS.
The promulgation of Decree 35 of the NHIS in 1999, marked the formal establishment of the scheme and its initial launch with the aim of providing UHC for all Nigerians using financial risk protection mechanisms by 2015.
However, the years that followed were marked by administrative inefficiencies and poorly implemented pilot programmes such as the University of Nigeria pilot which aimed to test the NHIS model within tertiary institution but lacked the necessary legislative backing and strategic planning to ensure long-term success. However, the scheme eventually began implementation on June 6, 2005.
Despite provisions for the formal and informal sector, and the vulnerable group in the scheme, the NHIS only covered about about 5% of Nigerians mainly federal civil servants while over 70% of health spending was financed through out-of-pocket payments.
The critical weakness of the scheme was its voluntary enrolment model which, despite allowing individuals the freedom to participate, consistently resulted in low participation. A 2013 study have shown that many people show apathy, even when participation is clearly beneficial, largely due to mistrust, limited awareness, or perceived lack of value.
The emergence of the National Health Insurance Authority
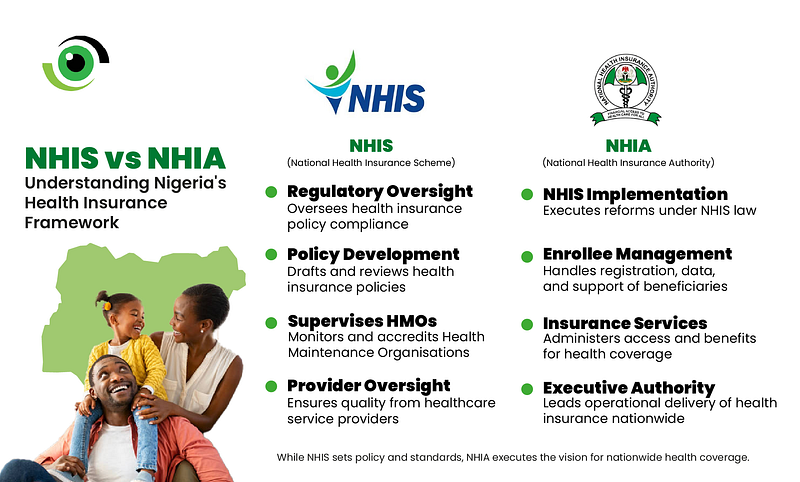
On May 19, 2022, President Muhammadu Buhari signed the National Health Insurance Authority (NHIA) Act into law.
The Act which repeals NHIS Act 2004, seeks to provide, promote and integrate health insurance schemes towards achieving UHC by 2030. The Act also established a Governing Council, composed of representatives from government agencies, organised labor, civil society organisations, and other relevant sectors specifically tasked with ensuring that health insurance is mandatory for all Nigerians and legal residents.
This provision represents a significant shift in Nigeria’s health financing landscape, as the Council is expected to develop an inclusive framework that accommodates all population groups, thereby advancing the goal of UHC. The council is also responsible for establishing a basic minimum package of health services to be uniformly applied across all health insurance providers in the country. Additionally, the NHIA provides general guidelines for the implementation and utilisation of the Basic Health Care Provision Fund (BHCPF).
A critical component of the Act noted that states in Nigeria, including the Federal Capital Territory (FCT), are empowered to expand access to healthcare for all residents by establishing a state health insurance and contributory scheme to cover all residents of the state.
This has led to the establishment and strengthening of already established State Social Health Insurance Agencies (SSHIA) which currently account for 50% of the total enrolment of health insurance. The Act also made available revenue mobilisation sources like the Vulnerable Group Fund (VGF) which aims to provide health coverage for approximately 83 million vulnerable and indigent Nigerians, which accounts for about 38% of the population. This represents a major expansion compared to the former NHIS, which covered less than 5% of the population.
Achievements of the NHIA
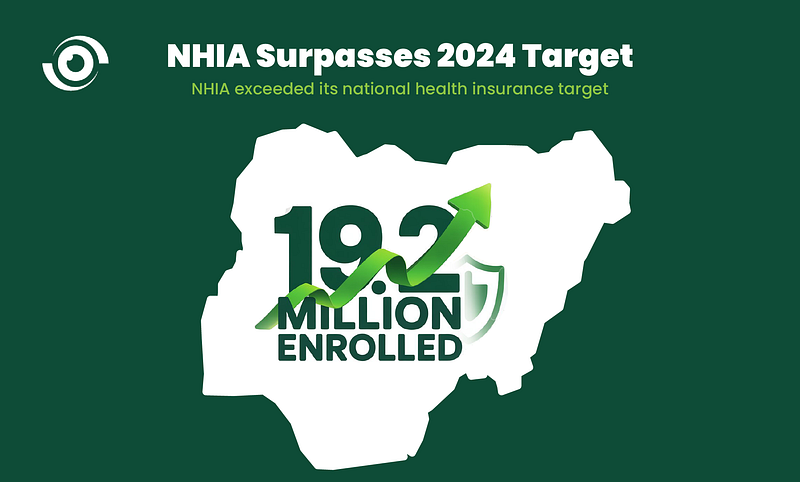
Through the deployment of these structures, the NHIA recorded 40% increase in health insurance enrolment from 16.7million to 19.2million in 2024. The NHIA implemented a temporary increase in capitation and fee-for-service (FFS) payments in July 2024 by 60% and 40% respectively as an interim measure to stabilise the healthcare sector and manage rising costs, pending the completion of a comprehensive actuarial review to establish sustainable rates.
If that elderly woman had presented with the same urgent orthopaedic need today, under the current structure of the NHIA, her experience might be different. With the recent 93% increase in capitation and a 378% boost in fee-for-service payments, health providers now have stronger financial incentives to prioritise insured patients and process claims more efficiently.
The NHIA’s digital systems and reforms also aim to reduce bureaucratic delays and improve turnaround times for approvals. This means that instead of waiting two days in pain, she could potentially receive approval within hours, start her treatment sooner, and avoid the deterioration that plagued her in 2021.
Reimagining her experience today, she might walk into a hospital, have her documents processed more swiftly due to improved claim systems, and receive surgery on time, all under a system better aligned with the core principles of UHC.
While these developments signal a positive shift in health insurance policy implementation, major structural and financial challenges remain, threatening the scheme’s long-term success.
Despite some increases in NHIA budgetary allocations, the percentage of the health budget dedicated to health insurance has remained critically low, never exceeding 0.11% over the last five-year period. This is grossly insufficient to cover a population of over 200 million.
Evidence from previous studies suggests that progress toward UHC is inversely related to the proportion of the population living below the poverty line. Although the NHIA model anticipates contributions from enrolees, the significant challenge remains that approximately 40% of Nigerians live below the poverty threshold and may be unable to afford regular premium payments.
Furthermore, there exists a significant inequity in access to healthcare services, particularly in rural areas and underserved urban communities, where most facilities are non-functional or below standard
A path forward
The NHIA Act holds considerable promise for transforming Nigeria’s health system. However, to achieve its full potential, it is essential for the Federal Government to increase health sector investments to at least 15% of the national budget, in alignment with the 2001 Abuja Declaration.
The NHIA Governing Council and state schemes should adopt transparent and practical revenue mobilisation strategies, including investment of funds, partnerships with regular donors and mechanisms for financial participation.
For the informal sector, alternative premium contributions such as in-kind or seasonal payments should be explored through accredited intermediaries such as cooperatives, market associations, or aggregators to collect and manage these alternative contributions. These entities must meet specific criteria, including good governance, accountability mechanisms, and digital reporting capacity Improving infrastructure and staffing in rural and underserved areas is crucial. State Primary Health Care Development Board, working with the National Primary Health Care Development Agency (NPHCDA), should rehabilitate neglected facilities and create incentives to attract and retain health workers in remote areas.
At the national level, retention of skilled professionals requires better working conditions, job security, and training expansion through collaboration between the Ministries of Health and Education.
Private providers are essential to system delivery and should be engaged through constructive dialogue and improved payment mechanisms. Strengthening their confidence in the scheme will enhance service reach.
Finally, managing population growth through expanded and guaranteed access to family planning and female education is key. Sustained public awareness campaigns, led by NHIA and supported by media and civil society, are essential to improve public trust and drive enrolment into the scheme.
1 Comment