
Kemisola Agbaoye and Mahdi Garba (Lead writers)
Haulat Abdulfatah, a 38-year-old mother of five had reservations when the campaign for the Human Papillomavirus (HPV) vaccine was launched in Ilorin East, a Local Government Area (LGA) of Kwara State. Despite her initial concerns, she brought three of her young daughters who were within the age group targeted by the vaccine, to receive the vaccination.
“Initially, I had reservations about the safety of the vaccine. But later, when the vaccinator explained to me that it protects young girls from cancer, I presented all my three daughters for the vaccine.”
Rukayyat Temitope another mother of five who had her only daughter vaccinated during the HPV vaccine rollout said she had seen several women close to her who suffered from cervical cancer.
“I know the benefits of the HPV vaccine,” she explained. “If I am to see people who are hesitant about taking the vaccine, I would use one or two scenarios as an example to make them allow their daughters to be available for the vaccine. The vaccine is safe.”

Abdulfatah and Temitope are two examples of caregivers who chose to have their children vaccinated as soon as the HPV vaccines became available in Kwara State. They were part of the campaign that led to the vaccination of over 300,000 girls across the state.
How it all began — Nigeria’s push for the HPV vaccine
The push to add the HPV vaccine into Nigeria’s National Programme on Immunisation (NPI) started in 2015, driven by the need to protect girls and women from the deadly threat of cervical cancer, which claims approximately 8,000 deaths annually. However, it was not until October 2023, that the initiative became a reality, with the launch of the first phase of the vaccine rollout, which targeted 7.7 million girls.
“The loss of about 8,000 Nigerian women yearly from a disease that is preventable is completely unacceptable,” Professor Muhammad Ali Pate, the Coordinating Minister of Health & Social Welfare, mentioned during the introduction of the vaccine into the country’s Routine Immunisation programme. “Cervical cancer is mostly caused by Human Papilloma Virus (HPV), and parents can avoid [the] physical and financial pain by protecting their children with a single dose of the vaccine.”
In Nigeria, cervical cancer is the third most common cancer and the second most frequent cause of cancer deaths among women between 15 and 44 years old, second only to breast cancer. The HPV vaccine has been commercially available since 2006 and was recommended by WHO in 2009.
“I’m sure you also know the HPV vaccine is one of the most expensive vaccines. In fact, it is the most expensive vaccine that the country has introduced” said Elizabeth Hassan, Senior Technical Officer and HPV vaccine and National Desk Officer for the HPV Vaccine Introduction at the Department of Disease Control and Immunisation, National Primary Health Care Development Agency (NPHCDA).
The cost of introducing the HPV vaccine is compounded by Nigeria’s large young population and the fact that the vaccine is targeted at school-aged children, distinguishing it from other routine childhood vaccines in the NPI. As a result, logistics and supply chain considerations for its rollout required new or additional structures.
Nigeria opted for the single-dose Gardasil-4 vaccine, targeting girls aged 9 to 14 years, in response to limited resources and the need to protect this vulnerable group from cervical cancer. This decision was unanimously endorsed by the Nigeria Immunisation Technical Advisory Group (NGI-TAG), following the announcement of the efficacy of single-dose vaccines by the World Health Organization (WHO) Strategic Advisory Group of Experts on Immunisation (SAGE).
Designing and implementing the rollout
The National Primary Healthcare Development Agency (NPHCDA), with the mandate for implementing Nigeria’s routine immunisation schedule, vaccine introduction and other vaccination campaigns, established an HPV Technical Working Group (TWG) to plan the introduction of the vaccine. This TWG was multisectoral, comprising a range of stakeholders, including donors, partners, civil society organisations, the media, and community leaders. These TWGs were also replicated at the subnational level.
“We worked with the Ministry of Defence, the Ministry of Education and the Ministry of Information as well as the press. And that is not excluding all our partners, CBOs and all the other NGOs that work in the space of maternal and anything related to female health. It was one of those vaccines that actually opened our eyes to a whole lot of stories. The introduction of the HPV vaccine has put us on a better pedestal to better implement future vaccines because now we have the full cooperation and collaboration of other ministries and we work closely together,” noted Dr Garba Ahmed Rufai, Director, Disease Control and Immunisation, NPHCDA.
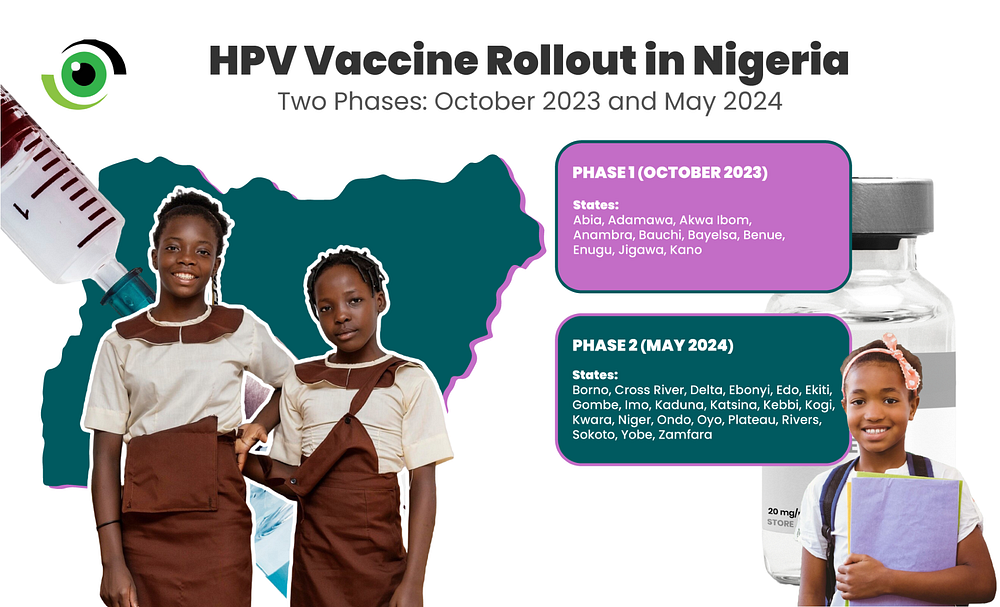
The rollout was implemented in two phases: the first phase in October 2023, in 16 states and the second phase in May 2024 in 21 states. This approach was designed to optimize resources and apply lessons learned from the first phase to the second phase of the rollout. One of the biggest challenges encountered during the first phase was the rapid spread of misinformation, both online and offline. In the first phase, efforts to counter and respond to anti-vaxxer tactics on social media proved ineffective and only amplified the misinformation. However, in the second phase, the approach shifted to “owning the story”, with the development and dissemination of strong narratives about the vaccine’s need, safety and efficacy on platforms where misinformation was spreading.
“This is the year we had the highest anti-vax [movement] in Nigeria. The last time we had this was in 2003 the Polio campaigns, it now came again in 2023 and spread into 2024 where there were misinformation and rumours. it was well orchestrated and well organised this time they made videos in different languages, in English, in different dialects of Yoruba. We also had those coming from outside the country. We had medical doctors coming out to address them,” added Dr Garba. “Radio houses became scientists suddenly and they knew more about vaccines than everybody else and they were telling different stories without checking the facts or talking to the professionals.”
This re-strategising was key to the success of the second phase of the rollout, which saw over 7 million girls vaccinated in the initial Multi-Age Cohort (MAC) campaign. It included the first five days of mass vaccination outreaches and targeted young girls both in school and out of schoolgirls. This brought the total number of girls vaccinated during the second rollout to over 12 million, excluding facility-based vaccinations.
According to Dr Nusirat Elelu, the Executive Secretary of the Kwara State Primary Healthcare Development Agency (KWSPHCDA), in the phase 2 rollout, they were able to prepare and better strategise, learning from the experience of the phase 1 states.
Vaccines from bustling towns to rural communities of Kwara State
Abibat Asaju, the Local Government Immunisation Officer for Ilorin South LGA, attributed the success achieved in the uptake of the vaccine to the effective mobilisation and sensitisation activities carried out during the campaign. These efforts were led by the state’s TWG, comprising of stakeholders from the Ministry of Education, Parent Teachers’ Associations (PTA), the Association of Private School Owners, and government-owned schools. The campaign also reached local communities, where large gatherings were held, and included roadshows in communities and marketplaces.

Another key factor in the success of the vaccine rollout was the involvement of community leaders and champions. Alhaji Abdulmumin Ayoku, the traditional chief known as the Mogaji of Fate community and its surrounding areas, pointed out that whenever a health programme, like the rollout of the HPV vaccine, is introduced, the traditional council plays an important role in ensuring that the message reaches every parent and household. He also noted that traditional leaders understood the benefits the vaccine would bring to their daughters, which is why they supported its rollout.
“They [our communities] believe in us. They know that we cannot mislead them. They know that we are telling them the right thing. They know their daughters will benefit most from what we are telling them. That was why we recorded almost 100% success in the programme,” Ayoku asserts. “Other states can come to Kwara and learn about how we did ours so that they can do it in their own states too.”
Sarat Yunus Mojisola, the State Immunisation Officer at the KWSPHCDA, attributes the success of the high HPV vaccine uptake in the state to leadership and coordination. She recalls that the state’s TWG was established before the rollout of the vaccine. Advocacy visits were conducted to the Governor, Commissioner of Health and all the ministries, departments and agencies (MDAs) involved. Weekly meetings were also held and a robust Advocacy Communications and Social Mobilisation Communication (ACSM) strategy, ensuring their advocacy messages reached the grassroots and secured the support of traditional leaders. In addition, as part of the pre-rollout activities, KWSPHCDA organised several training sessions to build the skills of its staff at the state, local government, and ward levels.

According to Mojisola, since the flag-off of the HPV vaccine campaign on May 27, 2024, people have been trooping into various healthcare centres across the state to vaccinate their daughters who are within the target age range. Kwara emerged as one of the states with the highest coverage in the country, reaching 117% target population coverage, exceeding the state’s 80% initial goal.
Supply side issues — inadequate manpower, vaccine stockouts and exclusion of private facilities
Mojisola, however, mentioned the lack of adequate skilled manpower as a significant challenge in the rollout of the vaccine in Kwara State, as well as stockouts of the vaccine attributing it to the success of the awareness campaigns, so the demands for the vaccine exceeded the available supply.
Kwara was one of five states to experience such stockouts, according to Yusuf Yusufari, Interim Deputy Director, Immunisation and Disease Control at the Bill & Melinda Gates Foundation, Nigeria Country Office.
One of the reasons for this was gaps in the timeliness and completeness of vaccination data in the District Health Information System (DHIS2), which slowed decision-making for the redistribution of vaccines from low-performing to higher-performing states and delayed the estimation of facility-based vaccination rates.
The national rollout of the HPV vaccine targeted only public facilities, effectively excluding population groups who access care in private facilities. As a result, individuals that access private healthcare had to pay out of pocket to receive the vaccine in private facilities. The decision to focus on public facilities was made to ensure that the vaccines were available to the target population for free, as private facilities have been known to sell doses when they were included in previous vaccine rollouts, such as the Rotavirus vaccine despite receiving the vaccine at no cost from government’s cold stores.
Elizabeth Hassan believes this might change in the future, now that the HPV vaccine has been integrated into routine immunisation. However, this will be based on the memorandum of understanding between the NPHCDA and private facilities, which allows them to charge only administrative costs when administering routine vaccines. For now, however, the HPV vaccine remains free only at public (government-owned) facilities.
Demand side issues — parental consent, the role of men and vaccine refusals
Parental consent emerged as a key issue during the rollout of the HPV vaccine, particularly among schoolgirls. This challenge was anticipated and is in line with learnings from HPV vaccine rollouts documented regionally and globally. Girls whose parents did not provide consent were not vaccinated, which is why they accounted for only 39% of the total number of girls vaccinated during the MAC campaign. Awareness and sensitisation of male caregivers are paramount, especially in communities where women’s decision-making power is limited.
“There is over-concentration of our vaccination campaigns on the women. When I was reviewing some of our data, I realised refusal of fathers to give vaccines to children is a major factor that breeds non-compliance,” Dr Nusirat noted. “This is one of the major challenges. Because we are in an African setting where the consent of the fathers is very important in vaccination, and it is key that we expand our advocacy to involve our male caregivers and fathers to encourage them to give consent to our mothers to give our children life-saving vaccination,” she added.
There were also instances of vaccine refusals by certain religious groups reported at both national and subnational levels in the state. Some religious institutions insisted that prayer was enough to protect them and rejected the vaccine.
There were also reports of refusal among the nomads, who feared adverse events following immunisation (AEFIs), however after they were informed about the importance of the vaccine, they brought their daughters to receive the vaccine.
Despite the lessons learned from states in the first phase of the rollout, misinformation persisted, even affecting the state’s supplementary measles campaign. The similarity in the sites of administration caused caregivers to refuse the measles vaccine, which prompted intense public awareness and education outreaches to address the issue, according to Dr Elenu.
What happens next?
Now that the MAC campaigns are over, the vaccines are available at government-owned health facilities and are now being included in the NPI schedule for girls from the age of 9. While girls aged 9 to 14 can currently receive the vaccine, this will be revised to only 9-year-old girls, starting from 2025.
1 Comment