Without good data, we’re flying blind. If you can’t see it, you can’t solve it – Kofi Atta Annan
There are about 3.4 million Nigerians living with HIV- or at least that was what everyone thought. This figure was based on a prevalence estimate of close to 3%, derived from the last version of surveys conducted in Nigeria. This meant that despite finding and placing over one million people on treatment with antiretrovirals (ARVs), it was still estimated that over 50% of those infected with HIV did not know their status. As millions of dollars were spent by the Nigerian government and its partners to find more people living with HIV, the narrative was that “Nigeria was failing to live up to the challenge of HIV/AIDS”. But everyone working in the field believed something must be wrong. They were working hard, testing millions, yet not finding more cases, but the narrative of failure persisted.
Now, the results are in. Nigeria indeed does not have as many people infected as previously thought. The previous surveys were wrong!
The just-released results of the population-based HIV survey in Nigeria
During the announcement of the NAIIS r esults , President Muhammadu Buhari also launched the Revised National HIV and AIDS Strategic Framework (2019-2021). Photo source: NACA
Given Nigeria’s vast population, planning is critical for health systems to deliver. No system can deliver services appropriately if not well guided by data which requires an understanding of the factors driving the epidemic. In the absence of robust and accurate data, Nigeria’s response to HIV was said to be foundering. Uncertainty about Nigeria’s HIV prevalence was seen as a problem, especially given the significant resources that had been dedicated to testing for HIV cases and the budgets that have been allocated for treating people with HIV.
In Nigeria, as in most countries with generalised epidemics, these estimates of HIV prevalence were largely based on surveys for pregnant women who attended a selected number of antenatal clinics. While most countries moved away from these surveys or developed improved protocols, this change did not happen in Nigeria, despite the global criticism of this approach. The most recent national estimates were based on an antenatal clinic (ANC) survey conducted in 2014. In Kenya, HIV prevalence was calculated using the Kenya AIDS Indicator Survey, a nationally representative 2-stage cluster sample of households and South Africa previously used antenatal testing data, however as this was not representative of the country’s population, the HIV prevalence rate in the country has been calculated using a nationally representative population-based HIV survey for many years. Looking back, Nigeria really missed an opportunity by not building the national expertise required to deliver complex surveys, nor did we build a team sufficiently trained that can deliver on this over the years. We were the focus of debates at international conferences and there was not much confidence in the data that we produced. Yet, the response had to be funded- and if the surveys estimated 3.4 million people infected, we had to find the funds to treat 3.4 million people. So, when it became imperative to get the numbers right, we looked for an implementing partner to deliver in this critical survey for Nigeria.

Image credit: Nigeria Health Watch
Enter the new leadership of the National Agency for the Control of AIDS (NACA) in 2016,

Director-General of NACA, Dr. Sani Aliyu speaks on his experience delivering the largest ever population-based HIV/AIDS survey carried out anywhere in the world.
Putting together the largest survey in the world
The need for a nationwide population-based survey has been voiced by civil society
Over the last decades, we have greatly improved our fight against the HIV epidemic. From NAIIS (results), we can see that fewer Nigerians are living with HIV. We cannot celebrate yet, because many of them are not on treatment– President Muhammadu Buhari at the Presidential announcement of the results
We applaud the government’s effort in capturing key and timely HIV data in Nigeria, given the logistical challenges in the country. These survey results contain critical information for planning HIV response and treatment and scaling-up interventions. They have also provided an opportunity to better allocate resources. Given that we do not have as many people living with HIV in Nigeria as had been estimated, what are the implications for donor agencies who have so far funded over 90% of our HIV response? Will PEPFAR or the Global Fund
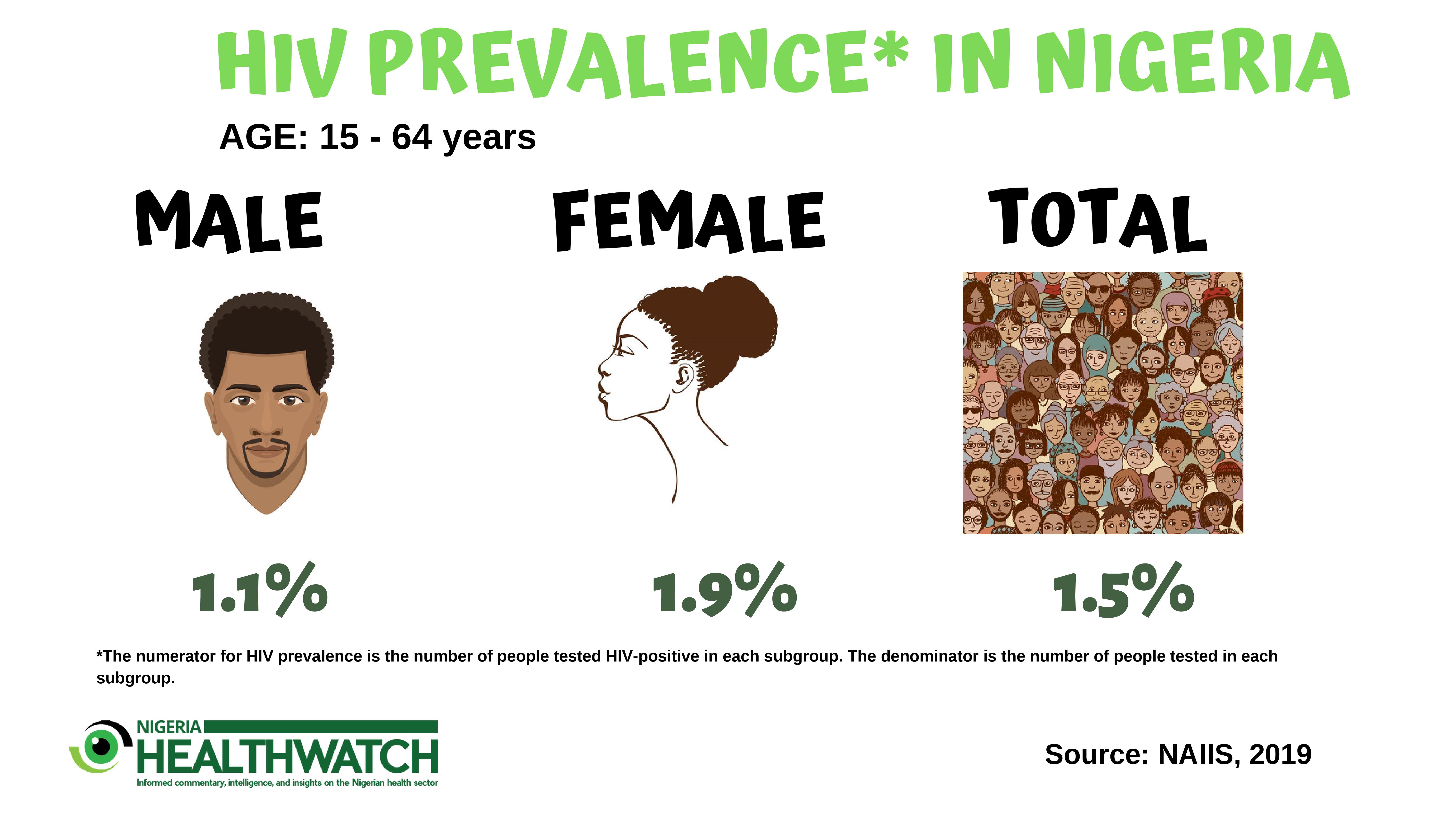
Women overwhelmingly bear the burden of HIV infection rates
According to the NAIIS result, HIV prevalence among women in Nigeria aged 15-64 is 1.9% and 1.1% among men. This prevalence figure is the same for women aged 15-49 years, however, for men, it is 0.9%. This implies that HIV disproportionally affects women in Nigeria. Could this be because of the inequalities that are driven by gender norms related to masculinity and feminism, violence against women, barriers of access to health services, poor education or lack of economic security? We would need to address some of these possible factors that put women at risk of HIV infections. For pregnant women who are living with HIV, it is important that we prevent the transmission of the virus from the mother to the baby. There is an urgent need for Nigeria to scale up prevention of mother-to-child transmission (PMTCT) services to be offered before conception, throughout pregnancy, delivery and breastfeeding. Family planning is one of the most vital PMTCT measures. Reducing the number of unintended pregnancies among women living with HIV would reduce the number of children born with HIV. States can play a large role in this by ensuring family planning services are provided in primary and secondary health facilities. In addition, now that we have state-specific prevalence data, state governments need to take more responsibility to employ better strategies that are needed to improve the accessibility, acceptability, affordability and uptake of HIV and reproductive health services, particularly for young women.
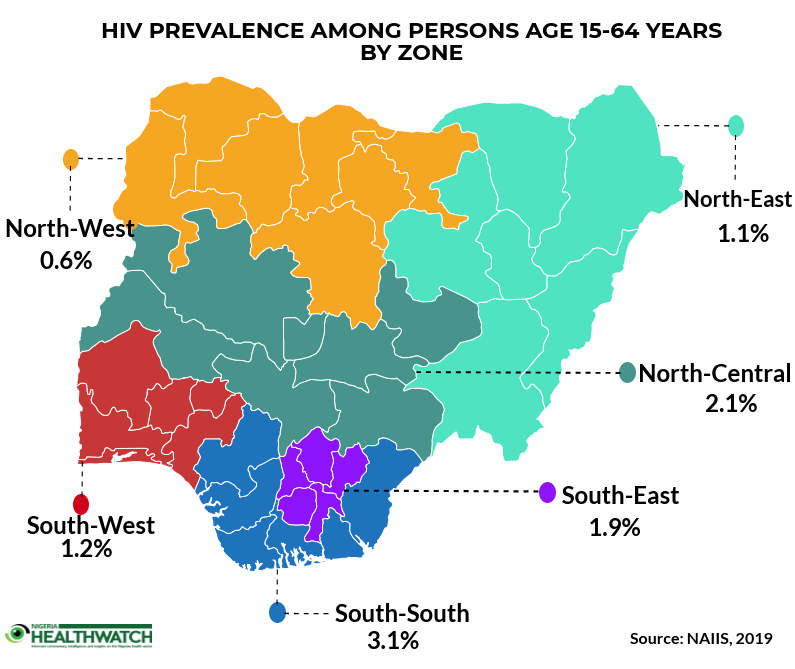
So where does HIV prevalence stand in Nigeria?
International donors and partners have dedicated significant resources to treating the previously estimated 3.4 million Nigerians living with HIV in Nigeria. The US government and the Global Fund spend $400 million and $110 million respectively every year funding the HIV response in Nigeria. Results from NAIIS have shown that HIV prevalence in Nigeria is 1.5% among people aged 1-64 years. This means that detailed discussions will now have to take place on what level of funding will come from our partners. For Nigeria to take greater responsibility for funding the treatment of people living with HIV in Nigeria, we must increase our total health budget. It costs about N50, 000 to treat a person living with HIV in Nigeria, for a year. In 2018, a total expenditure of N340.46bn was proposed for the Federal Ministry of Health. In order to accommodate the treatment of Nigerians living with HIV, it will most likely cost about two-fifths of the total health budget. If Nigeria is to develop a sustainable mechanism for funding HIV, we must consider integrating HIV treatment into national, state and community health insurance schemes. Our target should be for health insurance schemes to cover HIV treatment for its enrollees. Also, state governments need to take greater ownership for the HIV response in their states. If states could dedicate no less than 1% of their monthly federal government allocation to HIV treatment, it would go a long way in putting more patients on
Was it worthwhile spending $91million to have a clear idea of the number of people living with HIV in Nigeria? Absolutely, especially if we use this data to improve the response. The Government can now plan, develop and implement more effective programs to control HIV and Hepatitis in Nigeria, leading to healthier individuals and families. Since we now have a better estimate of HIV prevalence, we now call on our government to take greater ownership of the response. The next time we need to carry out a survey, we hope that we will not need an implementing partner to deliver on it.
How close are we to achieving the 90-90-90 goal?
UNAIDS has set the 90-90-90 target which would mean that by 2020, 90% of people living with HIV will know their status, 90% of people living with HIV will be on anti-retroviral therapy and 90% of people on anti-retroviral therapy will have viral suppression. These targets will all increase to 95% by 2030. However, the current viral load suppression among 15-64 is 44.5%, but given that population level viral suppression is essential, to say we have made progress in meeting the 90-90-90 goal, the viral suppression load should be closer to 73%. So, is there a silver lining? Given that the HIV prevalence rates are not as high as previous estimates, the country was failing to show the progress that had been made in tackling the HIV epidemic proportionate to the effort that had been put in preventing new infections. We are much closer to the first 90% than previously thought.
See photos from the presidential announcement of the NAIIS results here
This is good to know. We need to keep up the fight. Halt the spread and begin to reverse the trend.
We totally agree with you. The journey to an AIDS-free Nigeria begins now. We must not relent.
Timely and important, showing the effect of good leadership.
The scale of dearth of statistics and data of the Nigerian health system is the stuff of nightmares.
As graduate student, it was a huge pain to get data on disease processes in the country.
This makes for glad tidings indeed.
A very resourceful piece, thought-provoking for increased preventive actions by ALL.
Thanks for reading! Remember to share with your network.
Thanks for putting this together NHW. It was an exciting and fantastic read.Talking about the budgetary allocation for health, is it really difficult to simply increase it. and cut down on other expenses? I pray our arms of government take heed.
Thank you, Ebenezer, for your comments about the blog.
Nigeria signed up to the Abuja Declaration pledging to allocate at least 15% of the annual budget to health. So far, the country has allocated no more than 4%, so there lies the challenge. What this means is we will have to look to the private sector to contribute to funding for our health sector.
Understanding the “NAIIS” Survey and Critical Appraisal of the Survey.
Foremost, in the field of Public Health, professionals in the field are aware of the module called “URECA” (Understanding Research and Critical Appraisal). This module equips public health professionals to extensively review an article/research result such as the “NAIIS” survey result and critically analyze the article in order to help the public and users of the published article to understand the contents (facts & figures) and get informed about possible bias and information that could be misleading to the public and end users of the article/research results.
The “NAIIS” survey that was conducted recently in my country aimed to extrapolate the current national prevalence of HIV infection per state in the nation. A lot of resources (human, funds, technology etc.) were invested to make the survey successful and kudos to those field workers who made this possible.
Sequel to reading and digesting the published press release from UNAIDS on the NAIIS survey results, on a personal and professional note, I beg to disagree with the word “accurate” (as written in the published article) national prevalence of 1.4%. More suitable word would have been an “estimated” national prevalence of 1.4%. Other cited statistics in the article remain “accurate” until proven otherwise and they are most likely based on available data provided by stakeholders involved in the implementation of HIV/AIDs program in Nigeria right from the inception of HIV services in the country after the realization that there is high burden of HIV epidemic in the country, which was also based on a similar survey carried out many years ago and the national prevalence was pronounced as an estimate not an absolute or accurate figure of 2.8%.
There is no doubt that a lot of activities are ongoing in different regions and states in the country on the provision of HIV services, both on prevention and treatment. However, there are serious limiting factors to combating HIV epidemic across different areas within a state, region and nationwide, such as high level of discrimination and stigmatization in the society, low acceptability of positive HIV status due to beliefs and religion, poor medical care seeking behaviors, and socio-economic status. Even as HIV testing remains free in almost all public health facilities in the country, a lot of people are unaware and even many of those that accidentally got to know and after getting tested, realize their positive status, are scared of stigmatization and discrimination in the society, making it very difficult to accept and remain on treatment for the good of their well-being.
At the inception of free HIV services in the country many years back, with support from United States Govt., Melinda Gate Foundation and Global Fund, “serious” or a big magnitude of fear was unknowingly driven into the hearts of the populace through the media, inciting that “HIV/AIDs is incurable, HIV is this and that”. Though scientifically true, such media publicity that was aimed at informing people on HIV, so that people can come out, get tested and take treatment should not have had narratives that can discourage people from coming out voluntarily to get tested. The publicity across the country at that time drove fear into the hearts of millions, they rather not know their status till when its late and according to a national cliché, “na something go kill man” or “man must die one day”, millions of people refused to know their status even till now that the nation is meant to believe that HIV burden in Nigeria has greatly reduced from a prevalence of 2.8% to 1.4% – 50% reduction over a period of 20years+, based on the NAIIS survey that, though had a scientifically proven methodologies, but did not capture certain areas with recorded high positivity yield in different regions as part of the sample size in the survey. Rural communities like Ute, Uyere & Obadokun in the southwest region have high positivity yield, which is as a result of the existing culture & tradition compounded with poor awareness on HIV/AIDS and lack of free HIV services provision in the basic healthcare centre in those rural communities.
Aside the real low turnout by people in Nigeria to access free HIV preventive services such as HIV testing, millions still do not have access to HIV testing because of their location. In addition, aside the data-related decline in HIV prevalence in the country, the rate of incidence of new HIV infection across the nation is still a cause for concern.
According to the article, the statistics given on national viral suppression rate for those on treatment points to the fact that more people on treatment are virally unsuppressed which inversely could suggest that new HIV infections among the populace are dangerously looming or already at an alarming rate, coupled with the fear of stigmatization and discrimination in the society. In addition, the statistics on the number of people known to have been tested for HIV is insignificant to the estimated figure of Nigeria’s population. And if out of the millions that have been tested, an estimate (about or over) of 1.9 million people are living with HIV. That, in my opinion, affirms the existing burden of HIV in the country. Nigeria’s population is quite large and will require more resources internally and externally in order to achieve national epidemic control.
It is quite unfortunate that HIV data indicates that women are more affected as a result of the known higher risk due to women’s biology and this alone is a good reason for every stakeholder including the 3 tiers of government to take most seriously the imminent dangerous outcomes, if epidemic control is not achieved sooner than later. 20 years of HIV services is a long time and yet, based on statistics, over 60% of Nigeria’s population are either scared of knowing their HIV status because of stigmatization or do not believe that the system will protect their human rights to live without discrimination. More work needs to be done.
As much as I may want to be proud that my nation is said to be on the track to HIV epidemic control, I also fear that Nigerians living with HIV, on free treatment or not on treatment at all, may soon lose the magnanimous support from international bodies and when that happens, I can only say it will be well.
Recommendations
Strict national policy on the fight against HIV stigmatization and discrimination in the society especially at workplace and healthcare facilities, private and public.
Extensive grass root publicity with encouraging messages, tailored to promote early detection and treatment and the good outcomes of starting treatment early. There is good life even if you are HIV positive, so far you are on treatment. There many other diseases that are worse than HIV and more debilitating to live with.
Educative and informative interventions that will aim at changing the perspectives of people towards people living with HIV, just as almost everyone has a family member or friend living with other chronic diseases like high blood pressure, diabetes etc.
If possible, special resources to be allotted to special circumstances such as when there are people diagnosed with HIV who cannot afford the little expenses that they need to cover to access the “currently” free treatment at certain designated health facilities in their rural communities or state or region across the nation. Expenses such as transportation fare to reach distant facilities where there is free treatment, payment for basic laboratory investigations that may be necessary prior to commencing treatment, payment for antenatal services in case of a poor pregnant positive woman and payment for delivery services as required by many secondary and tertiary health facilities.
Heart warming that Nigeria produce credible data on HIV/AIDS. Kudos to the new leadership at NACA. Please extend this new seriousness in data collection to other bogus health data that given the country a wrong image. Well done.
Thats a good job.At least a good decision can be taken with such data
Thank you, Ebenezer, for your comments about the blog.
Nigeria signed up to the Abuja Declaration pledging to allocate at least 15% of the annual budget to health. So far, the country has allocated no more than 4%, so there lies the challenge. What this means is we will have to look to the private sector to contribute to funding for our health sector.