
Ibukun Oguntola and Oluoma Omeje (Lead Writers)
Providing access to healthcare is widely recognised as a fundamental human right, as outlined in the Constitution of the World Health Organization (WHO), which states that “the enjoyment of the highest attainable standard of health is one of the fundamental rights of every human being”.
The 1978 Alma Ata declaration, brought global attention to the goal of “Health for All” establishing it as central priority in public health. The concept of Universal Health Coverage (UHC) gained momentum in 2005 and was further strengthened by a World Health Organization resolution and publication of the World Health Report in 2010. For the first time, it considered three dimensions — population coverage, service coverage and financial coverage or protection.

The push for UHC gained further momentum in the 20th and 21st centuries, particularly in the global health landscape, with the United Nations and other international organisations playing a key role in promoting it as a priority. Even the idea of ensuring access to healthcare can be traced back to ancient societies, demonstrating the long-standing recognition of the importance of health for individuals and communities.
This raises an important question: Even though countries recognise the importance of UHC as a means to improve health access, why has it been difficult to achieve especially in low — and middle-income ones?
In addition, fragmented knowledge sharing exacerbates the challenge. As countries struggle with limited mechanisms for documenting and exchanging successful practices, opportunities for learning are frequently missed.
Even when there is awareness of global best practices, adapting these lessons to local political, economic, and cultural contexts remains a hurdle. The complex interplay between global UHC strategies and local realities demands a tailored approach that encourages local ownership and sustained technical support. The very notion that “its extremely difficult to translate literature or global best practices into our own context” is at the heart of the challenge low- and middle-income countries face.
The Joint Learning Network for UHC
The Joint Learning Network (JLN) for UHC arose from the urgent need for a more collaborative, country-led approach to solve these challenges. Established in 2010 during early discussions on UHC, the network was born when a small group of countries including India, Thailand, Philippines, Ghana, Vietnam and Kenya met on the sidelines of a global health convening in May 2009 to discuss the need for cross-learning among countries working towards UHC, recognising that they were working through similar obstacles.

As Kadarpeta explained, “the idea of having a platform to regularly discuss about certain aspects of universal health coverage implementation came naturally when we realised we were addressing similar challenges and could learn from one another.”
Under the network, JLN member countries share information and ideas and develop solutions and tools to support health system reforms and achievement of UHC. The JLN currently includes 40 member countries across Africa, Asia, Europe, and Latin America as well as 12 non-member countries participating in JLN collaboratives, working together and sharing experiences through multilateral workshops, country learning exchanges, and virtual dialogues.
In one illustrative moment, Rahul Kadarpeta, “We had to come together and exchange our ideas, to share what was working and, just as importantly, what was not working.”
This process not only distills complex global policies into actionable field advice but also supports members by transforming shared experiences into co-produced knowledge products ranging from toolkits to policy briefs that are grounded in real-world practice.
JLN distinguishes itself by being wholly country-driven. Rather than relying on traditional top-down technical assistance, the network harnesses the tacit knowledge of its member countries. As Kadarpeta described, “the synthesis of new knowledge is primarily from country experience it comes directly from our senior policymakers and practitioners who are on the ground.”
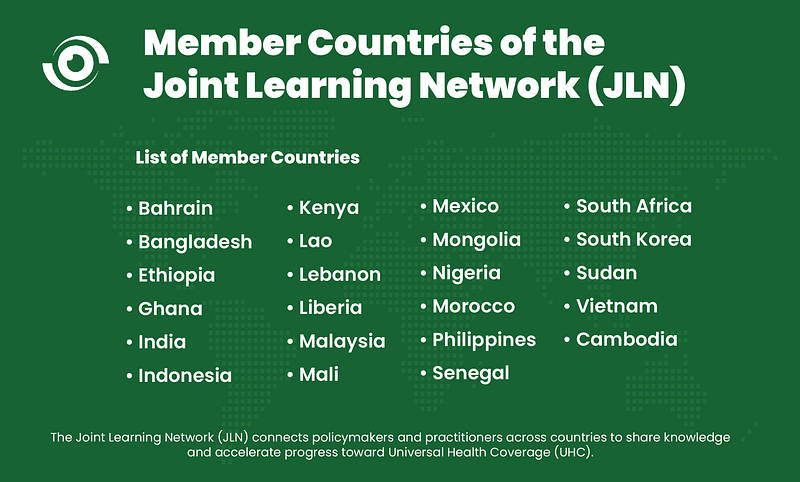
*In total, JLN now has 41 members, of which 23 are full members (presented here) and 18 are associate members.
Every member country forms a Country Core Group composed of key stakeholders including officials from the Ministry of Health, national health insurance agencies, finance ministries, technical partners, private and civil society organisations. These groups not only set the learning priorities, but also elect the network’s steering group to govern its agenda.
Senior policymakers and practitioners have noted that despite the focus around modern health financing, “it was very difficult for policymakers and practitioners to translate what UHC-related strategies like provider payment mechanisms, strategic purchasing, public finance management, and other mechanisms actually mean on an operational basis,” Dr Rahul Kadarpeta, Executive Director, the Joint Learning Network for UHC (JLN) shared. This perfectly encapsulates the struggle to transform abstract policies into practical, context-specific actions.
Collective problem solving
Over the past decade, JLN’s model has generated measurable impact across low and middle-income countries:
- Practical Learning and Application: JLN has facilitated over 40 themed collaboratives and learning exchanges, resulting in co-production of 45 practical tools. These tools, such as case studies and toolkits, help countries “quickly put together a policy note” following a study visit or country pairing engagement.
- Widespread Utilisation: JLN tools have been downloaded more than 8,000 times across at least 94 countries, including 69 non-JLN member states. These tools have also be utilised beyond member states to contribute to global guidance from organisations like the World Bank and WHO.”
- National and Regional Transformations: Countries such as Ghana (since 2010), Kenya (since 2011), and Nigeria (since 2011), have seen tangible policy impacts from the JLN. “There is this Direct Facility Financing in Nigeria that is an outcome of JLN, along with reforms in Primary Healthcare,” Kadarpeta noted.
- Scaling Engagement: With over 75 participating nations, three-quarters of which are low — and middle-income countries, and more than 400 technical experts engaged across sectors, JLN’s network has a striking reach and inclusivity.
Evolving global health dynamics
Understanding that the thematic areas at the heart of UHC reforms are inherently dynamic. What worked in 2012 might not be effective by 2020, as country system dynamics evolve.
One key dynamic that JLN continues to address is the turnover of policymakers and practitioners at the country level who have shaped the network over the years. As leadership transitions occur, whether through retirement or promotion, key individuals who have long championed JLN’s work in the countries move out of the system, sometimes limiting continuity of the strategic vision.
Reflecting on this challenge, Kadarpeta said to keep up with new leaders coming in, we conduct consistent orientation on the JLN ways to maintain the network’s continuity, especially as new entrants must familiarise themselves not only with JLN’s core principles but also with the decorum required to sustain its safe space for open discussions. Mentorship from our JLN Champions is always supportive.”
One key observation within JLN is the differing levels of progress among member countries. Some nations have been part of the network since its early years, working through foundational reforms and advancing into complex, emerging areas such as climate-related health policies, digital health innovations, emergency preparedness, and artificial intelligence applications in healthcare.
In contrast, newer entrants into the JLN, such as Burkina Faso, Botswana, Lebanon, Mali, and South Sudan, are just beginning to address foundational UHC challenges that older member countries started to tackle nearly 15 years ago.
This natural progression of countries through their development cycle requires a tailored approach to knowledge sharing within the network. Simply applying the same strategies used by early adopters may or may not work for newer members, given the varying economic and institutional contexts in which they operate. To address this, JLN is considering strengthening its country pairing model and learning exchanges for small groups of countries, where nations with extensive experience in UHC reform are actively paired with newcomers for direct, regionally relevant exchanges.