


Tzar Oluigbo (Lead writer)
Aisha (not her real name) had been in labour for over two days in Tula, a remote community in Kaltungo Local Government Area (LGA) in Gombe State. By the time a referral was made to the State Specialist Hospital in Gombe, after prolonged obstructed labour that the facility could no longer manage, she was exhausted.
The journey to the hospital, which took a few hours, felt even longer given her condition, with exhaustion, labour pain, and fear weighing heavily on her. For Aisha, each delay was a dangerous gamble with her life and that of her unborn child.


“When she arrived, we did everything we could to stabilise her,” recalled Usman Aliyu, desk officer for the Comprehensive Emergency Obstetric and Newborn Care (CEmONC) programme at the hospital. “We had prepared to take her in for surgery,” he noted; however, “in that critical moment, as we rolled her into the theatre, the power went out.”
The anaesthesia machine used during the surgery depended on electricity. Without it, the team had no choice but to refer her again, this time to the Federal Teaching Hospital in Gombe, about six kilometres away. Aisha pleaded not to be moved, having already come a long way. “Please find a way to save me here, don’t refer me,” Usman recounted how she begged. Unfortunately, Aisha died before she could reach the Federal Teaching Hospital.
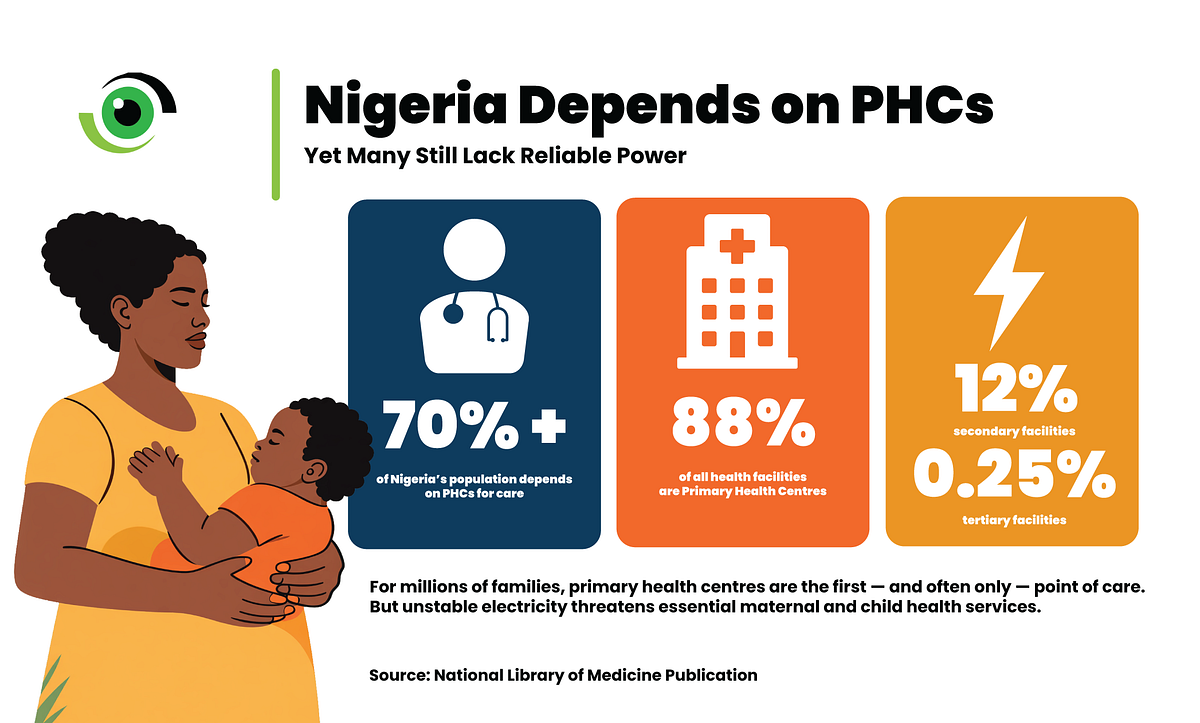
Reliable electricity is a fundamental requirement for safe healthcare delivery, yet it remains a significant challenge in many low-resource settings, including Nigeria. A joint report estimates that nearly one billion people rely on health facilities that either have no electricity at all or must manage with unreliable power.
In Nigeria, the situation remains particularly difficult. Approximately 40% of functioning primary health care (PHC) facilities lack access to electricity, and less than 20% use solar power. Frequent power outages and rising energy costs, worsened by a 200% increase in electricity tariffs, have forced some hospitals to dedicate up to a quarter of their operating budgets to electricity. Almost half report that unreliable power has affected the quality of care.

In 2020, the Rural Electrification Agency (REA), through the Nigeria Electrification Programme (NEP), installed a 50-kilowatt solar-hybrid system at the Gombe State Specialist Hospital as part of efforts to strengthen healthcare services through reliable energy access.
The system now supplies power to critical units throughout the facility, including the Intensive Care Unit (ICU), the Main Theatre, the Gynaecological Theatre, and the Accident and Emergency Unit. With continuous electricity, essential services, particularly emergency obstetric and newborn care, can now be provided without delays or risks caused by previous power interruptions.
When power determines survival
Before the solarisation of the Gombe State Specialist Hospital, unreliable electricity was one of the main barriers to providing timely care for mothers and newborns. Emergency surgeries were delayed or interrupted, oxygen-dependent equipment could not operate, and even routine procedures became challenging in the darkness.
In the maternity complex, health workers improvised. “There were times we used torchlights, hunters’ lamps or even kerosene lamps to conduct deliveries,” explained Sarigamo Ibrahim, a nurse and midwife who manages the maternity unit. “Sometimes the torch would go off, and if we couldn’t get any phones to use, we had to wait till morning to continue.”


In a facility performing 150–200 deliveries monthly, including up to 26 in a single night shift, with about 10–15 requiring sutures, these interruptions carried deadly consequences. Cases of postpartum haemorrhage (PPH) were not managed quickly enough, leading to severe blood loss and preventable deaths. Sarigamo explained that “even with severe perineal and cervical tears, we couldn’t suture properly without light. Those tears can lead to heavy blood loss and even death.”
Babies born with birth asphyxia, a condition where a baby does not receive enough oxygen before, during or immediately after birth, which accounts for an estimated 900,000 deaths each year, cannot be helped. Blood samples could not be processed on time. The system was fragile, and lives were lost in the gaps.
Powering critical care
Electricity is not just about lighting; it supports nearly every aspect of maternal and newborn care. From storing life-saving drugs like Oxytocin to powering incubators, oxygen concentrators, and surgical equipment, reliable energy ensures continuous, timely care. “Now, even if the main power goes off, the solar takes over immediately,” Sarigamo explained.
“There is no interruption. We can suture, we can operate, we can do everything.” For newborns, this difference is critical. “In cases of birth asphyxia, we use machines that depend on electricity to help babies breathe. We used to record over 50 neonatal deaths monthly, but now it has reduced to about 20 to 25,” she said.


Over time, staff observed a significant improvement in maternal and newborn outcomes. “Before the solarisation, we used to record between 15 to 20 maternal deaths monthly, but now we hardly record more than one or two in a month,” Sarigamo said. “Last year, we recorded about five maternal deaths in total. It is still painful because every life matters, but the reduction is considerable.”
Despite progress, challenges persist
Dr Sambo Jones Dawa, the Chief Medical Director of the Gombe Specialist Hospital, noted that the intervention has significantly improved service delivery and reduced avoidable deaths linked to power disruptions.
However, “our burden for service delivery has increased because most people no longer go to those private clinics. 60% of the clients come to Gombe Specialist Hospital because it is centrally located, we have the cheapest rates, and there are no protocols like the Federal Teaching Hospital, which affect wait times.”
The increased patient load has stretched available staff. In some wards, a single nurse may care for over 20 patients. Training gaps and the need for more modern equipment also persist. “With more patients coming in, the workload is overwhelming,” Aliyu, Desk Officer for the CEmONC, noted. “We still need more manpower and continuous training.”
As more facilities turn to alternative power solutions, the lesson becomes clearer: improving health outcomes is not only about medicines, personnel, or equipment. They rely on something that patients rarely see. When the power fails, service delivery is interrupted, surgeries pause at a critical moment, and a newborn’s breathing may need to be supported by hand. In maternity care, this becomes harder to manage safely. Health workers are then forced to make very difficult decisions in real time, often with very limited options.
This is where power policy and health outcomes intersect, with direct implications for economic productivity, reinforcing that a reliable power supply and health cannot be planned in isolation. Keeping these systems running determines whether care continues, and patients receive the treatment they need in a safe environment. As more facilities invest in reliable power, the added cost is placing further strain on an already stretched health system.