
“Formal education will make you a living; self-education will make you a fortune.” Jim John
Continuous capacity development is integral in healthcare service delivery and administration. But to be able to meet up with the continuously evolving and demanding expectations of the complex Nigerian healthcare system, healthcare professionals, policymakers and administrators must keep building their capacity both to be effective and to be exceptional in their responsibilities.
The challenge for most healthcare professionals is finding training designed with the right mix of relevant content and practical execution methods. For capacity building programs to be effective, they need to be tailored to meet the unique healthcare context of participants and the communities they serve. They also need to be experiential by using evidence and delivery methods with which participants can relate.
One training model that has shown promise in being able to combine these two factors is the Leadership Enhancement and Accountability for the Public Sector (LEAPS) Programme. The programme targets administrators and policymakers from health governance institutions to build their quality improvement, leadership and organizational management skills. Organized and delivered by the Healthcare Leadership Academy (HLA), the 2018 edition of LEAPS held recently in Abuja. The LEAPS programme runs a fellowship model that commences with training, followed by mentorship, where the HLA team mentors participants for a period of time to ensure they apply the skills they have acquired.


Image credit: Nigeria Health Watch
Here are six interesting things that healthcare training designers can learn from the successes of the LEAPS programme.
1. Adaptability & Responsiveness are key for training programs
Understanding how to adapt programs to meet changes and respond to real-life situations is a critical factor for training programs to consider. The more responsive a training program is, the better it is able to meet the needs of those who go through the program and the more efficient it becomes. The LEAPS Programme in its last edition had included an 18-month period for participants to carry out their post-training interventions.
Dr. Omoh Duze, the Programme Manager for LEAPS pointed out that they observed that some of the teams in the 2017 cohort were able to complete their interventions in eight to nine months as opposed to eighteen. As a result, they decided to make the intervention period 8 months in the 2018 edition.
2. Ensure buy-in from senior executives
Health interventions are not executed in isolation. The buy-in of senior leadership of the healthcare institutions is an important factor that can impact the success or failure of project
interventions, and so senior leadership are important targets for health training programmes if learnings are to be implemented post-training.
The HLA team observed that some of the participant teams in its 2017 group had challenges with getting the support of their state executives when they returned to their places of work
To prevent this from happening in 2018, HLA organized the State Executives Leadership Programme (SELP) prior to the LEAPS programme, providing an opportunity to engage with the senior leadership of the different Health Ministries, Departments and Agencies (MDAs) from which LEAPS participants would be drawn. The leadership who participated in the SELP helped select and prioritize the projects to be implemented by LEAPS participants. This made them fully aware of the projects the teams would be working on when they returned from the training, and as a result, increased the amount of support they would receive from senior leadership.
3. Foster interagency collaboration
Adopting a multi-stakeholder approach in healthcare interventions is often lauded on paper but neglected in practice. This leads to silos in efforts, the reinvention of the proverbial wheels, duplication of efforts, and a waste of limited funds. Interagency collaboration is one way to stem these challenges, and the LEAPS programme found ways to do this.


The participants from the current cohort were strategically drawn from three states, Niger, Nasarawa and Kaduna. Photo source: LEAPS
All states had representatives from the State Ministry of Health (SMoH), State Primary Health Development Agency (SPHCDA), State drugs and medical supplies management agency, and the state budget and planning commission. The SMOH need the SPHCDA to implement their plans because they operate at the grassroots level. Also, the availability of essential medicines and commodities in primary health centers is critical to the success of most healthcare interventions and above all, these plans and projects need funds which are not available. “The State Budget and Planning Commission needs to understand the importance of all line items and advise the planners if their budgets are realistic”, Dr. Duze said, while explaining the rationale for participant selection. “Everyone is important.”
4. Encourage Experiential and Evidence-Based Learning
Experiential and evidence-based learning allows training participants to be immersed in their learning environment, to learn by doing, and to instantly plough back lessons learned into future work because it involves practical and hands-on learning.
For the LEAPS Programme, ten participants from each of the three states were put into two teams. The two teams focus on a project already selected by their superiors during the SELP and this forms the basis for all their learning. The projects are derived from each state’s already existing Annual Operational Plan (AOP).
This process provides an immersive learning environment because participants are basically doing the same thing they would be doing at the end of the training exercise. They are able to ask important questions to understand the significance of the project and what evidence is available to support the rationale behind the particular intervention.
5. Ensure accountability from participants
Making sure that participants in training are able to step down their knowledge is an important aspect of health training programs that those who design training should take into consideration. This allows participants to fully embrace the training programme and prepare to guide others once they are back in their work environments.
The HLA team say they make an intentional effort to have participants step-down their training to colleagues.
Even though the teams work on their project plans throughout the training, they are not expected to single-handedly implement them when they get back to their workplaces. They are expected to guide the process and provide oversight responsibilities to their subordinates. As a result, leadership coaching is a key component of the training as it equips participants with skills to elicit better performance from their teams.
6. Understand how to prioritize health interventions
Helping health policy makers and planners understand how to prioritize health interventions in the face of competing needs and issues as well as assessing challenges to interventions will go a long way in making a training program achieve its objectives.
The LEAPS programme deployed two tools to help its trainees better prioritize health interventions. The first is what it called the “2 by 2 Matrix” which assesses the potential impact of an intervention and the level of challenge anticipated in order to achieve it. Challenges could include capacity gaps, finance, or infrastructure, amongst others.
The second tool is the Driver Diagram, which helps policy makers and health planners think through and connect their project aims to primary and secondary drivers needed to make them work. The interventions and strategies needed to make the secondary drivers work form most of the activities of the intervention.

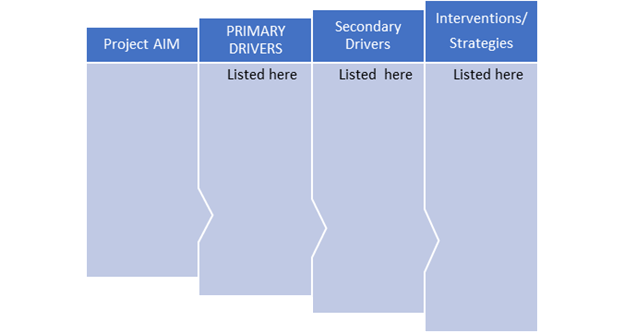
Image credit: Nigeria Health Watch
Participants at the 2018 Edition of the LEAPS training were excited about the impact they felt the training would have on their job performance. Mr. Joseph Barde, Deputy Director of Planning, Research and Statistics at the Niger State Ministry of Health, said the training will improve their productivity because tasks are taken from already existing action plans of the participating states. He said the leadership and team management aspects of the training will improve their work because of the different types of people they work with.
Designing targeted and tailored programs such as this will obviously take a lot of resources, but it is worth the time and investment to ensure participants are gaining skills relevant to their unique contexts and learning in ways that are practical, efficient, and effective.
Very good.
Leadership, quality improvement and evidence-based practices are some of those emerging subjects that our health workers need to build their capacity in order to provide quality care and ensure patient safety.
Other areas where we need to build the capacity of all health workers are infection prevention and control, and antimicrobial resistance and stewardship; both areas are of global concern to help us address the scourge of infectious diseases and antimicrobial resistance, locally, nationally and internationally.