
Safiya Shuaibu Isa (Lead Writer)
The Nigeria Health Sector Renewal Investment Initiative (NHSRII) and its ambitious 4-Point Agenda represent a comprehensive roadmap aimed at building a more responsive, equitable, and resilient health system, with the ultimate goal of achieving Universal Health Coverage (UHC) and improving population health outcomes.
Significant financial commitments, including over ₦2.48 trillion from the 2025 federal budget and $3 billion from development partners, are underpinning efforts to revamp service delivery, including the upgrade of primary healthcare (PHC) facilities nationwide.
A renewed focus on accountability is also evident through initiatives like aligning state and federal operating plans and real-time digital tracking. However, the overall intent and efforts above can only make sense to the end-user when they translate to satisfactory service delivery at health facilities.
Translating health policies into tangible improvements in service delivery at the community level has historically been a challenge in Nigeria. Issues such as a lack of political will, poor leadership and governance, funding gaps, and fragmentation within the health sector have often hindered effective implementation after policies and approvals are in place.
The disconnect between PHC and people-centred care
While Nigeria has a network of almost 33,000 PHC facilities — constituting the majority of healthcare establishments — the ratio of facilities to the population remains unbalanced, and geographic access does not always equate to actual service utilisation.
Many PHC facilities are underutilised, largely due to perceived poor quality of services and a fundamental mismatch between the available care and the actual health needs expressed by the population.
There is a disconnect between the health needs and aspirations of the people and the services provided. Historically, PHC was conceived as an intervention programme for the rural poor, focusing on priority diseases and preventive care using non-professional workers. This approach did not align with the population’s need for comprehensive, quality health care, which includes curative services.
The vulnerable and low-income earners have a right to professional-quality healthcare and are not content with intervention programmes catering to selected diseases. This perspective is important in understanding the gaps in the journey between policy ambition and the reality of service delivery.
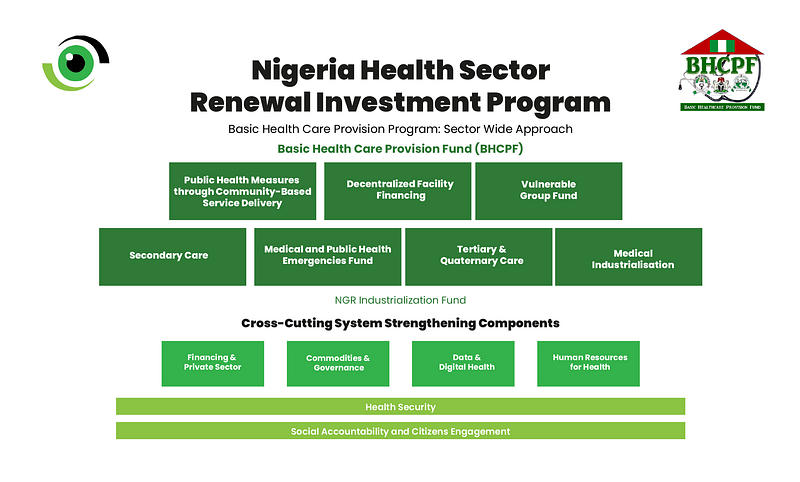
The Sector-Wide Approach (SWAp) is being emphasised as a strategic tool within the NHSRII framework to address fragmentation and build a truthful, resilient, and effective health system. SWAp aims to foster coordination, transparency, and accountability.
Nigeria’s ongoing experience with the NHSRII is presented as an opportunity to write a different story compared to past efforts that faltered due to bureaucracy and a disconnect from implementation. However, sustaining the progress requires not only continued political will and data-driven implementation, but a deeper engagement with both frontline workers and the communities they serve. Simply put, people will only use the care or service they trust.
Listen to respond
In March 2025, Nigeria Health Watch conducted a Community Listening exercise across six focal states: Lagos, Niger, Ebonyi, Borno, Kano, and Cross River. The process employed a multi-stage cluster sampling technique to ensure geographic and demographic representation, offering a granular, data-driven view into how Nigerians experience and perceive PHC services.
The findings offer a fresh lens on progress under the NHSRII and reveal a complex, state-specific mix of trust, dissatisfaction, and reform readiness. While PHCs remain the first point of care in most rural communities, urban residents, especially in Lagos, are increasingly bypassing them in favour of private hospitals.
Notably, across the board, citizens want one thing: affordable, available, and respectful care. However, they are not experiencing it equally. The insights derived from community voices are vital for deepening subnational implementation, restoring trust in public health services, and bridging the disconnect. Ultimately, success will depend on how equitably services are delivered and whether citizens feel seen, heard, and served.
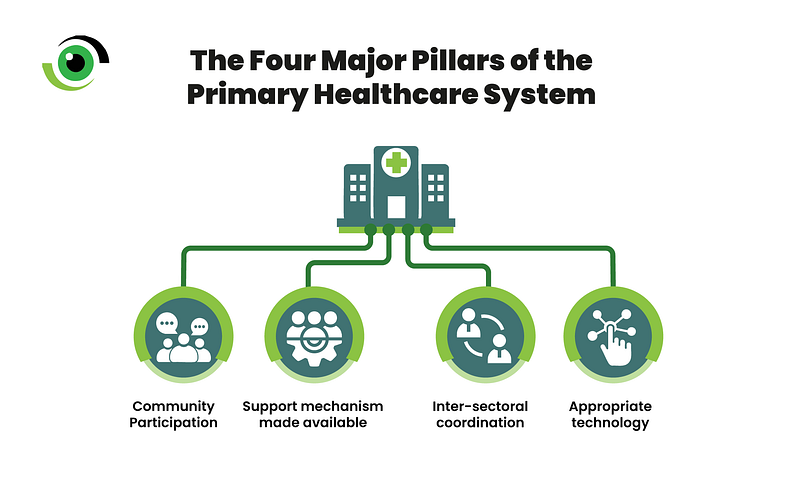
Nigeria needs to strengthen the primary care movement that prioritises community engagement and leverages the active participation of health professionals, civil society organisations (CSOs), community leaders, the general public, and even Nigerian health professionals in the diaspora. The goal of this movement is to educate and mobilise stakeholders to bring people back to the centre of PHC and to overcome political inertia.
Recommendations from CSOs, such as the Nigeria UHC Forum, a coalition of diverse CSOs, for strengthening the NHSRII framework include increasing accountability to and participation of relevant stakeholders and Nigerian citizens.
Some African countries’ experiences offer valuable perspectives on how community engagement and civil society involvement can be effectively leveraged to improve accountability, service delivery, and trust in PHC at the community level.
In Kenya, community engagement is considered a critical success factor for the deployment of Primary Care Networks (PCNs), which are designed to achieve UHC. This engagement is facilitated through the Community Health Workforce. Community members are directly involved in decisions regarding the use of health facility revenue through Health Facility Committees.
Evaluations have shown that involving community representatives in managing facility funds can strengthen transparency and community involvement, leading to improved health worker motivation and patient satisfaction. Kenya also plans to institutionalise social accountability mechanisms, such as the Community Score Card, specifically to empower communities and hold PHC providers accountable for service quality.
Nigeria has laid a strong foundation with the NHSRII and the adoption of the SWAp, but moving from policy to tangible action in PHC delivery requires deliberate efforts to listen to community voices and include feedback in the design and delivery of PHC, strengthen community engagement, and leverage the power of civil society.
By amplifying citizens’ voices, fostering accountability through transparent mechanisms and citizen oversight, building genuine partnerships with communities and civil society organisations, Nigeria can enhance service delivery, rebuild trust in its PHC system, and accelerate progress towards improving health outcomes and UHC goals. This inclusive approach is not just desirable, but essential for the successful transformation of primary healthcare in Nigeria.
The subject title caught my attention (Listening to respond) and really sparked my interest to read it all through. A lot needs to be done to improve Primary Healthcare (PHC) and make it accessible to the people. I hope NHSRII will actualize its four-point roadmap agenda, bringing it to life beyond just a plan. Health Watch should just keep Watching.
Nice read!