
‘Delivering a baby is what gives me joy the most’, explains 26-year-old midwife Aliya Lawal Adam as she takes time out to attend to her one-year-old daughter, her third child, outside the delivery room of the Akilu Memorial Hospital, the only Primary Health Centre (PHC) in Unguwar Galadima, Madobi Local Government Area, Kano State. Aliya and another young lady, Fatima Iliyasu, both in their mid-20s, are the only two graduates of Community Midwifery in their Local Government Area (LGA). Around midday on this sunny Friday afternoon, the two ladies attend to a woman in labour in the delivery room of the PHC. They have worked at the PHC for the past 8 months.
The Community Midwifery course is designed to focus on the provision of midwifery services at PHCs in the community. It was adopted by health training institutions with the support of Women for Health, a non-governmental organisation working to improve maternal and child health in six Northern Nigerian states; Katsina, Yobe, Zamfara, Jigawa, Borno and Kano. Aliya and Fatima are also among the 42 graduates of the course in Kano state, all from rural areas.
The young ladies were selected with the help of their community leaders, screened and trained in a one-year foundation program before being enrolled in a two-year study program. They graduated in April 2018 and have been providing maternal health services at facilities in their area. For Akilu Memorial Hospital, the health worker in charge, Mallam Isah Abdullahi says the work of Aliya and Fatima has led to improvements in antenatal visits and facility deliveries by women in the area.

Some of the final year students of nursing at the katsina state school of nursing. Photo credit: Nigeria Health Watch
The case for more female health workers in Northern Nigeria
The lack of trained health workers in health centres across rural communities is one of the factors that discourages women from attending antenatal and postnatal care, as well as giving birth in health facilities. A shortage of professional health workers such as nurses and midwives often leads to Environmental Health officers and Laboratory Technicians providing services such as antenatal care and delivery services in some facilities.
Mr. Idris Zubair, Director of Nursing and Midwifery services at the Kano State, Ministry of Health mentioned that even when health workers are available, socio-cultural sensitivities in northern Nigeria means that the thought of a woman being attended to by a male health worker is not traditionally accepted. Yet, a large proportion of girls from rural communities do not have the chance to further their education beyond secondary school. Health workers are also reluctant to work in facilities located in rural areas, often due to the working conditions. This combination of scenarios has contributed to a huge dearth of skilled female health workers in the north of Nigeria, compounding the country’s already poor maternal and child health indices.
According to the latest Multiple Indicator Cluster Survey (MICS), antenatal coverage in the North West and North East of Nigeria is at 53.6% and 67% respectively, compared to South West and South East regions which have 89.5% and 91.3% coverage. Delivery at the health facility is not any better, with the North West at 17.8% and North East at 25.8% compared to 87.5% in the South East and 76.6% in the South West. The percentages from these regions contribute to Nigeria’s high maternal mortality ratio of 814 per 100,000 births and under five mortality rate of 104 per 1000 births.

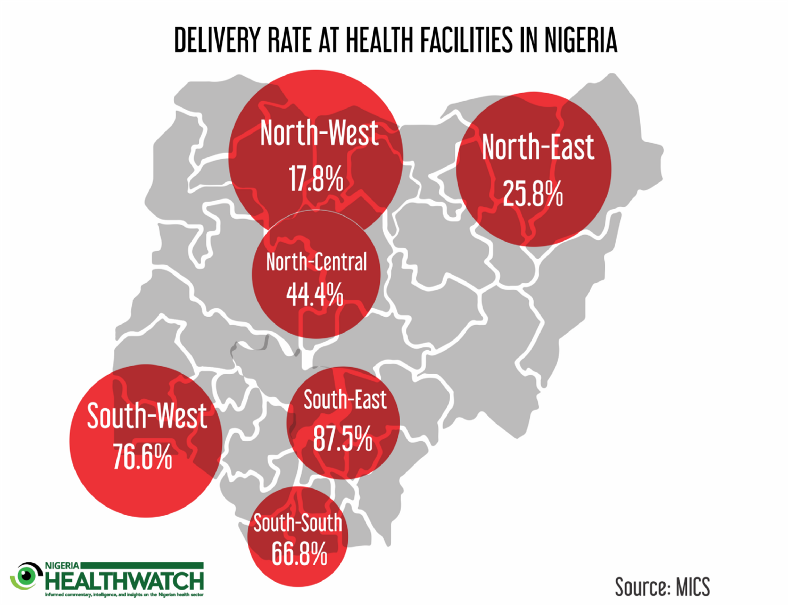
Image credit: Nigeria Health Watch
A promising HR stop-gap for rural healthcare in Nigeria?
Training more female health workers in rural health facilities, most critically in underserved communities, could be a game changer in the drive to encourage more women to give birth at PHCs, especially in northern Nigeria. This is the goal Women for Health had in mind when in 2012 they entered into agreements with 6 states to help train young women as midwives and nurses.
In each state, they surveyed communities that did not have female health workers in their PHCs. They then liaised with community leaders in those communities to identify young women who had completed their secondary school education. The young women were then screened and tested and the top three candidates from each local government was trained in one of the institutions in their state to become either a nurse, basic midwife, community midwife or community health extension worker (CHEW). They signed an undertaking that stipulated that upon graduation, each candidate would return to her community to serve for a minimum of two years.


Community midwife Fatima Kabir providing family planning counseling to a mother of six at Comprehensive Healthcare Centre Mashi, Katsina State. Image source: Nigeria Health Watch
Women for Health provides the students with hostel accommodation, meals and a stipend of N5,000 monthly during their foundation year, during which they are taught new subjects. Upon passing the entrance exam and gaining admission to the course, their school fees and other course requirements are paid by Women for Health, while they continue to receive a stipend. The initiative has enabled over 290 young women from rural communities in Kano State to be trained as health workers, producing 42 community midwives, 23 community health extension workers, 28 basic midwives and 2 nurses. The rest of the students are either going through their studies or are enrolled in the foundation year program.
Homegrown healthcare delivery… with a feminine touch
Further up in Panshekara area, a rural suburb outside Kano city, lives 27-year-old Fatima Ibrahim, a basic midwife. Thanks to the Women for Health program, Fatima is the first girl in her family to go beyond secondary school education. She graduated in March 2017 and since then has been serving not just in the PHC a few kilometres from her family house, but also as the first port of call for women in the immediate community.

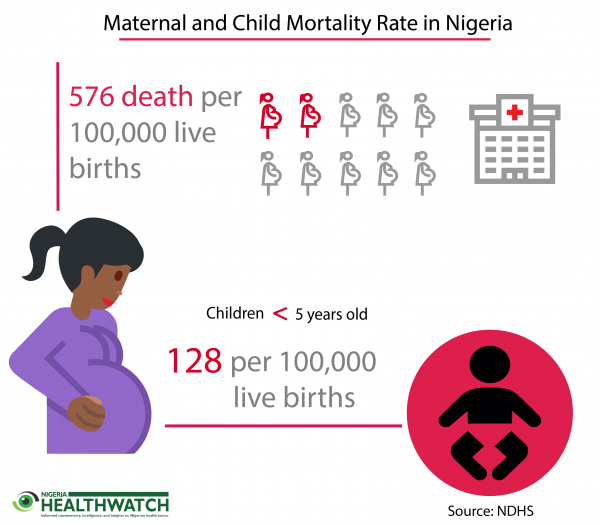
Image credit: Nigeria Health Watch
‘People knock at my door in middle of the night requesting her to go and see their wives in labour’, a smiling Malam Ibrahim Musa, Fatima’s father, says. He takes such pride in his daughter that he now wants her to proceed to university and become a medical doctor. Aside counselling on family planning, healthy living during pregnancy and breast feeding, Fatima has been assisting women in her community to deliver their children, especially at night. About a month ago around 3 a.m., she assisted her neighbour Amina Yakubu when she gave birth to a girl she called Zainab.
Along one of the roads that connects Kano to Katsina State, through Daura town, is a comprehensive health centre in the town of Mashi, about 40 kilometres from the city of Katsina. Inside one of the rooms in the centre, 30-year-old community midwife Fatima Kabir counsels a mother of 6 who is almost the same age as her, about family planning. Kabir is married with three kids and is one of the only two community midwives in Mashi Local Government area. She is the only health worker from her community of Tsintsiya, north of Mashi. There is no health centre in her community, so she is posted to this centre, and has to take a motorbike every day to and from work. ‘Using family planning products will protect women from many complications that come with pregnancy and child birth’ she says enthusiastically before adding, ‘It is the service I love providing the most’ as she goes back to her client.
Kabir is one of the 38 community midwives that has graduated so far from the initiative in Katsina State, out of over 400 young women from different rural communities who have benefitted. Over the last year, antenatal and delivery attendance has increased dramatically at CHC Mashi, and the health worker in charge, Malam Dikko Lawal believes that Kabir must be given credit for having successfully completing the midwifery course. The biggest improvement, he says, has been deliveries at the facility. Before she joined them just over a year ago, not more than 10 out of the over 100 women that attended antenatal visits at the health facility came to deliver there, but in the last few months, the facility has been recording close to 100 deliveries per month, in addition to the up to 200 women that attend antenatal care every month. More women from Kabir’s community also attend antenatal and deliver their babies at the health centre. However, Kabir is now overworked according to Malam Dikko, as she works seven days a week, including at least three night shifts per week.

One month old Zainab delivered by community midwife Fatima Ibrahim in Panshekara area of Kano state. Photo credit: Nigeria Health Watch
Katsina State School of Nursing, which shares a fence with the General Hospital in the heart of Katsina city, is where 102 students from various rural communities of the state are receiving a one-year foundation year training. The training is aimed at introducing them to an environment of higher learning. Aisha Munir, 18, from Dangamau village in Kusada Local Government and her two friends, 19-year-old Amina Isa Audi from Bindawa Local Government and 18-year-old Fatima Iliyasu from Jibiya Local Government area cannot wait to finish the foundation year and start their training. They all want to pursue the Community Midwifery program because they hope to use those skills to provide antenatal care to the women in their respective villages, once they are done.
Will states garner the political will needed for continuity?
Women for Health’s intervention comes to an end in 2020, and beyond that, the 6 states must adopt, strengthen and work to sustain the programme. Katsina and Kano State governments have already taken over the programme from 2017, while Women for Health continues to provide technical support. While Katsina State has automatically recruited the students who have graduated and pays them a salary, the students from Kano State are still working as volunteers in their various communities, some have been doing so for more than two years.
The Director of Nursing Service in Kano noted that there are processes in place to absorb the midwife trainees into the civil service within the coming months. This is important to encourage the young women to continue giving their best and not to dent the morale of other young girls looking up to them in the community. In addition, the process of recruiting the girls through recommendation by community leaders could be prone to bias and favouritism, even though they undergo screening at the local government afterwards. More transparency could be ensured if every girl who feels she is qualified is allowed to put herself forward for screening after necessary announcements are made. Through this, the program will be less prone to possible vested interests.
Human resources for health is one of the most critical aspects of healthcare delivery, and nowhere is this more important than at the primary healthcare level, which is the foundation of any health system. As Nigeria continues to work to improve maternal and child health indices, attention must be given to nurture, train and retain health workers especially at the community level. Programs like the one being implemented by Women for Health give rural women the opportunity to receive healthcare from skilled healthcare workers who also happen to be women they are familiar with, in addition, the young women are now more economically empowered. These programs should be scaled up and provided with financial support by states intent on closing the human resources for health gap, especially in rural communities.
I’m so glad to see the impact this initiative is yielding. We can do more, we can achieve much more by designing home grown solutions for our problems. We can engage more of indigineous health workers to solve our problems. We can generate more political will. We can make nigeria better
Excellent intervention.
I hope state govts will take it up